Article Text

Statistics from Altmetric.com
Description
A 23-year-old woman with a diagnosis of diffuse large B-cell lymphoma presented with an area of erythema and discomfort in her lower back after administration of intrathecal chemotherapy (figure 1).

Skin reaction post intrathecal chemotherapy.
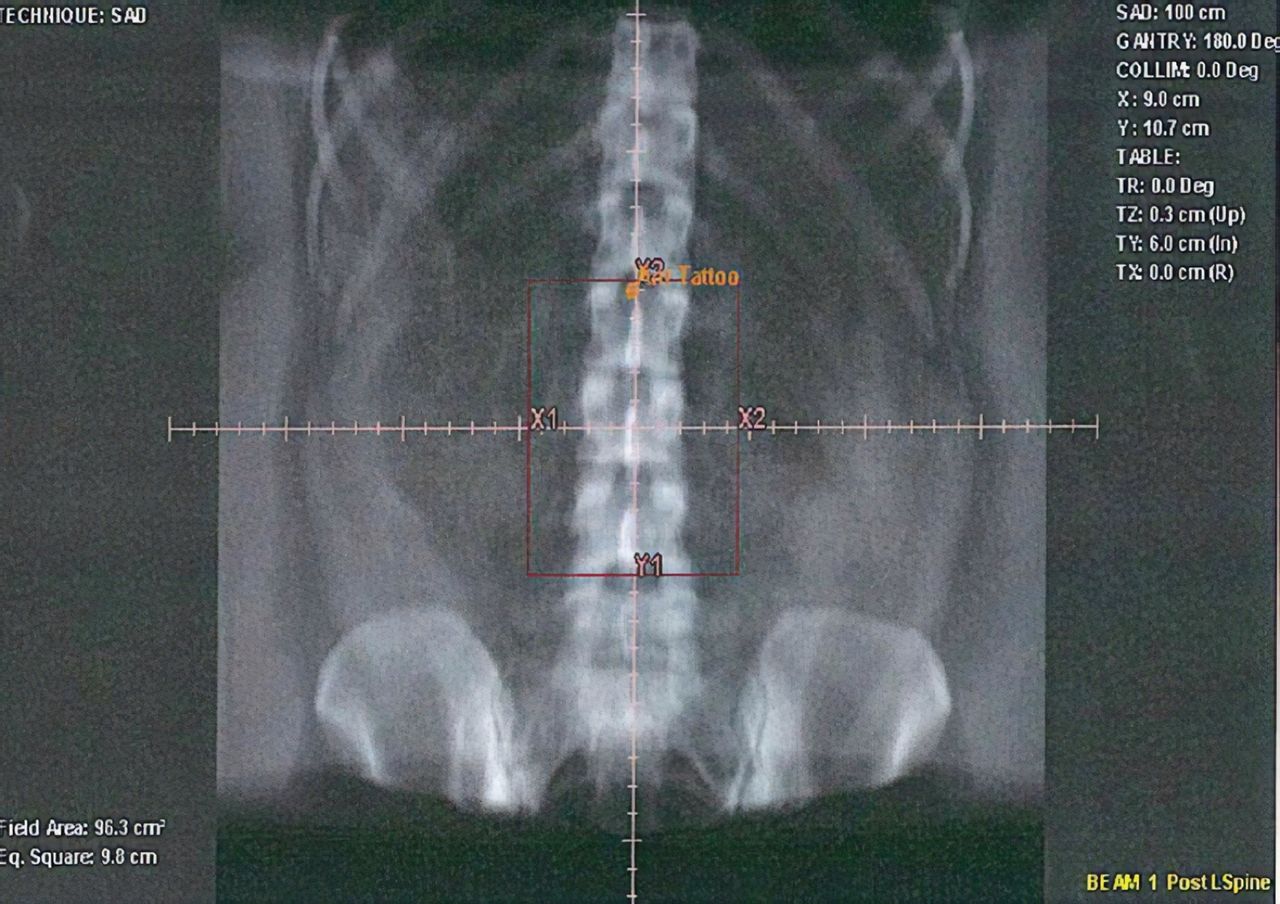
She originally presented with a 4-month history of back pain with leg weakness. MRI confirmed a pathological fracture at L3 which was encroaching into the spinal canal. She was treated for an impending cauda equina compression with a single 8Gy fraction of palliative radiotherapy, delivered to L2– L4 (figure 2). Subsequent investigations were consistent with disseminated diffuse large B-cell lymphoma.
{kind=link}
{kind=link}
Lumbar spine radiotherapy plan.
After initially being treated with R-CHOP chemotherapy, she was commenced on R-CODOX-M 6 weeks after completion of radiotherapy. She received intrathecal methotrexate as per the planned regime. Within a few hours, an abnormal area inferior to the intrathecal site was noted. This was initially attributed to extravasation. As the lesion further developed, advice from the oncology team was sought.
On examination, there was a well-demarcated rectangular patch of erythematous skin and one area of moist desquamation found in the midline of the lumbar spine, consistent with a diagnosis of radiation recall. Differential diagnoses included extravasation, contact dermatitis, eczematous reaction or other de novo skin pathology (ie, Bowen’s disease).
A diagnosis of dressing-induced contact dermatitis was excluded due to being able to visualise the intrathecal site distal to this region and determining that the location of the dressing was therefore also distal to this (in addition to a different shape). For this reason, extravasation could also be excluded. Erythema, moist desquamation and warmth, clinically indicate a skin inflammation and reaction, and with the uniform shape seen, this shape thereby raised the suspicion of radiation recall (rather than a de novo skin lesion or eczema). Her radiotherapy plan was reviewed and the area of skin reaction corresponded precisely to the area previously treated, with the location, size and shape matching the measurements documented on the reviewed radiotherapy plan.
General supportive advice was given for the skin reaction (eg, regular emollients and dressings as required). With these conservative measures, the reaction improved and subsequently resolved.
Radiation recall is a recognised complication of radiotherapy in up to 6% of patients, in which patients can experience delayed acute inflammation of the skin within the field of previous irradiation. This is thought to be triggered by chemotherapy, more commonly described with anthracyclines, antimetabolites, taxanes and methotrexate.1 Radiation recall can be distinguished from acute radiotherapy toxicity according to the time of onset, >7 days or <7 days respectively with a median time of 39 days.1 2 Pathophysiology is not yet proven.
Learning points
Radiation reactions can occur late, in response to systemic therapy.
Utilising acute oncology service or specialist nursing teams with clinical uncertainty in specialist fields.
Acknowledgments
Andrew Brown - Macmillan Clinical Nurse Specialist for Acute Oncology Services at Maidstone Hospital
References
Footnotes
Patient consent for publication Obtained.
SLF and JG contributed equally.
Contributors All authors have had equal participation in co-authoring and reviewing of article. SLF andJG: planned, concepted and designed project, performed acquisition and analysis of evidence, wrote and reviewed report. CM: planned and designed project, reviewed, revised and critically appraised project; provided supervision and guidance with final approval.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.