Article Text

Statistics from Altmetric.com
Description
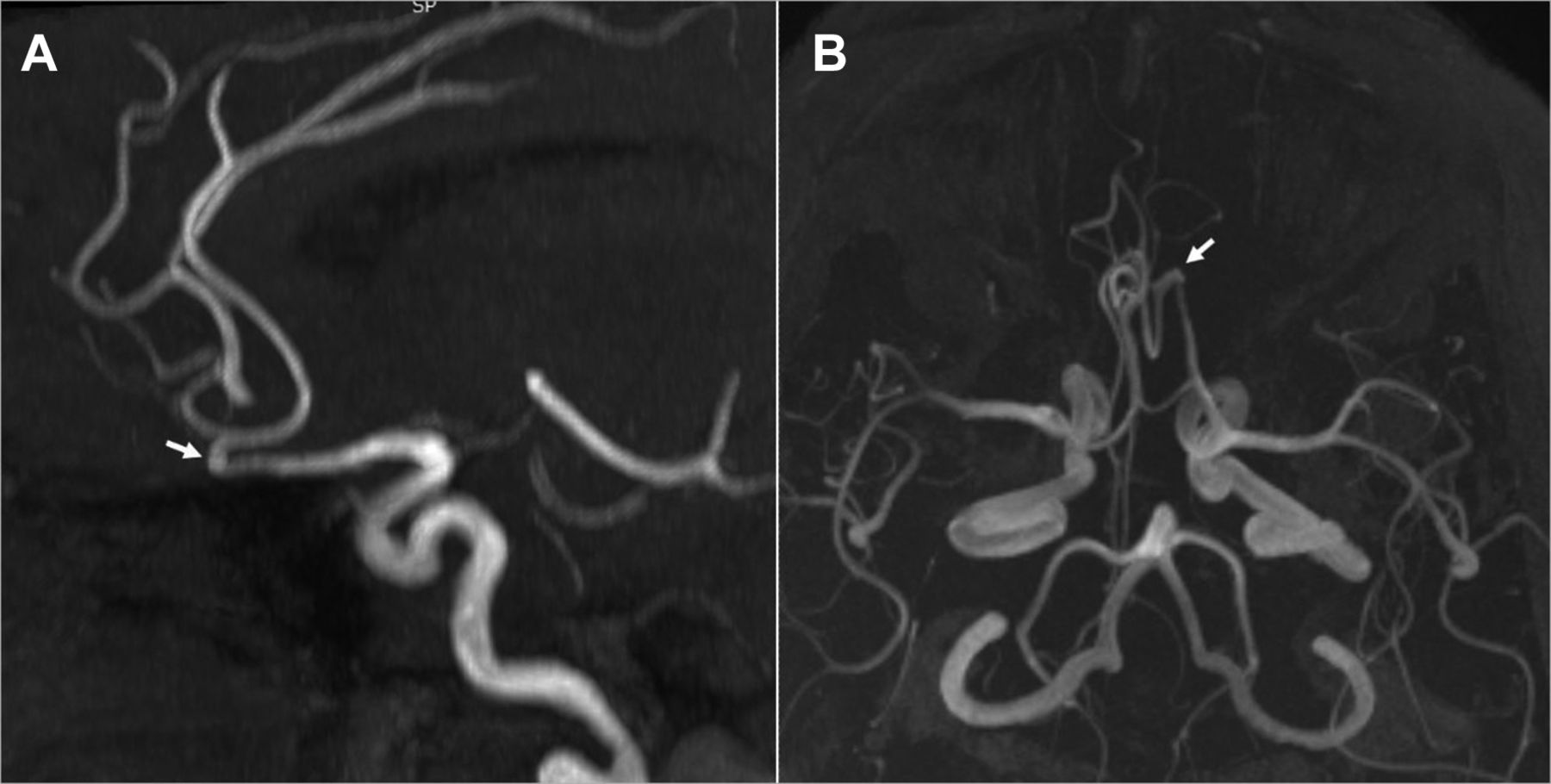
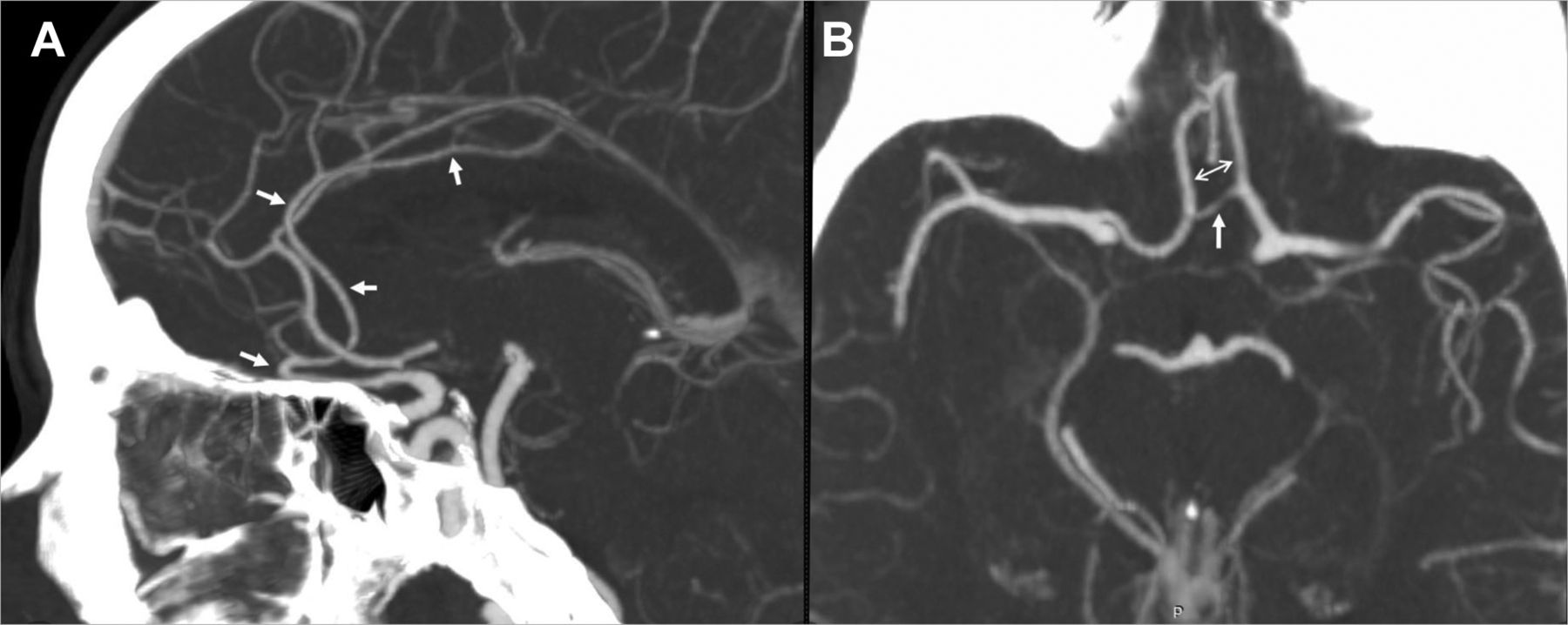
A 58-year-old woman presented with a severe headache without a history of seizure or neurological deficits. She was evaluated for subarachnoid haemorrhage. MR angiogram (figure 1) showed a hairpin curve of an anomalous artery in the location of left anterior cerebral artery (ACA). In its cranial course, it continued as pericallosal artery, supplying the left ACA territory. A long anterior communicating artery (AComA) widely separated it from right ACA. Corroborative CT angiogram (figure 2) with its superior resolution, established the absence of recurrent artery of Heubner as well as an aneurysm. Thus, a diagnosis of left persistent primitive olfactory artery (PPOA) was made, and our patient was advised follow-up imaging.

Three-dimensional time of flight MR angiogram showing paraolfactory hairpin curve (white arrow) of left persistent primitive olfactory artery in oblique sagittal view (A) showing rostral continuation of left persistent primitive olfactory artery as pericallosal artery to anterior cerebral artery territory and craniocaudal view (B) showing elongated anterior communicating artery.

{kind=link}
{kind=link}
CT angiogram: (A) sagittal maximum intensity projection image showing left persistent primitive olfactory artery course (white arrows) in relation to anterior cranial fossa, hairpin curve continuation to pericallosal artery. (B) Axial MIP image of cranial CT angiogram showing widely separated persistent primitive olfactory artery and A2 segment of the right anterior cerebral artery (thin arrows) and long anterior communicating artery (thick arrow) with absent recurrent artery of Heubner.
PPOA is a rare variant of ACA with 0.14% incidence, mostly reported in the East-Asian population.1 Embryologically, it results from non-involution of the cranial division of primitive internal carotid artery. Out of the described variants, first is an intracranial continuation as pericallosal artery after a paraolfactory hairpin curve, as seen in our case. The second variant shows transcranial continuation as ethmoidal artery supplying the nasal cavity. A transitional variant, branching out to continue as both the pericallosal and the ethmoidal arteries is described by Horie et al.2
An aneurysm at its hairpin curve, resulting from the haemodynamic stress is found to be the most common cause of clinical presentation; anosmia related to altered olfactory nerve perfusion has also been implicated rarely.3 Three-dimensional TOF MR angiogram suffices to initially diagnose the PPOA and in its follow-up. CT angiogram is helpful to demonstrate the status of artery of Heubner, AComA and aneurysm with higher sensitivity.
Learning points
Persistent primitive olfactory artery is a rare variant of anterior cerebral artery with a hairpin curve before its cranial course.
It is associated with a vulnerability to develop an aneurysm at the acute curve due to haemodynamic stress.
Pre-emptive identification and timely follow-up imaging may aid prevention and elective management of associated aneurysm.
Footnotes
Patient consent for publication Obtained.
Contributors BH contributed in image acquisition workflow protocols, postprocessing and manuscript preparation. PS reviewed imaging, reporting and conceptualised the manuscript. AK and CKA reviewed imaging and provided intellectual contribution for manuscript preparation.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.