Article Text

Statistics from Altmetric.com
Description
Our patient is a 15-month-old Caucasian girl with antenatally diagnosed chromosome 13 triallelic mutation. She was born full-term with a birth weight of 2600 g and APGAR scores of 9 at 1 and 5 min of life with no significant perinatal illness. Our patient presented to the hospital frequently for recurrent respiratory infections. She also suffered from mild oropharyngeal dysphagia with weak swallows and coughing on feeding of fluids since birth. These were initially attributed to poor respiratory health and an antenatally diagnosed aberrant right subclavian artery resulting in oesophageal compression and chronic microaspiration.
As part of work-up for her swallowing dysfunction, a video fluoroscopy swallowing (VFS) study was conducted by the speech therapist and radiologist. In one of the images for which thin fluids was administered, a thin sliver of contrast medium is seen to enter the upper trachea from the upper oesophagus. A H-type tracheoesophageal fistula was suspected and the study was aborted. The paediatric pulmonologist and surgeon were emergently informed of this finding.
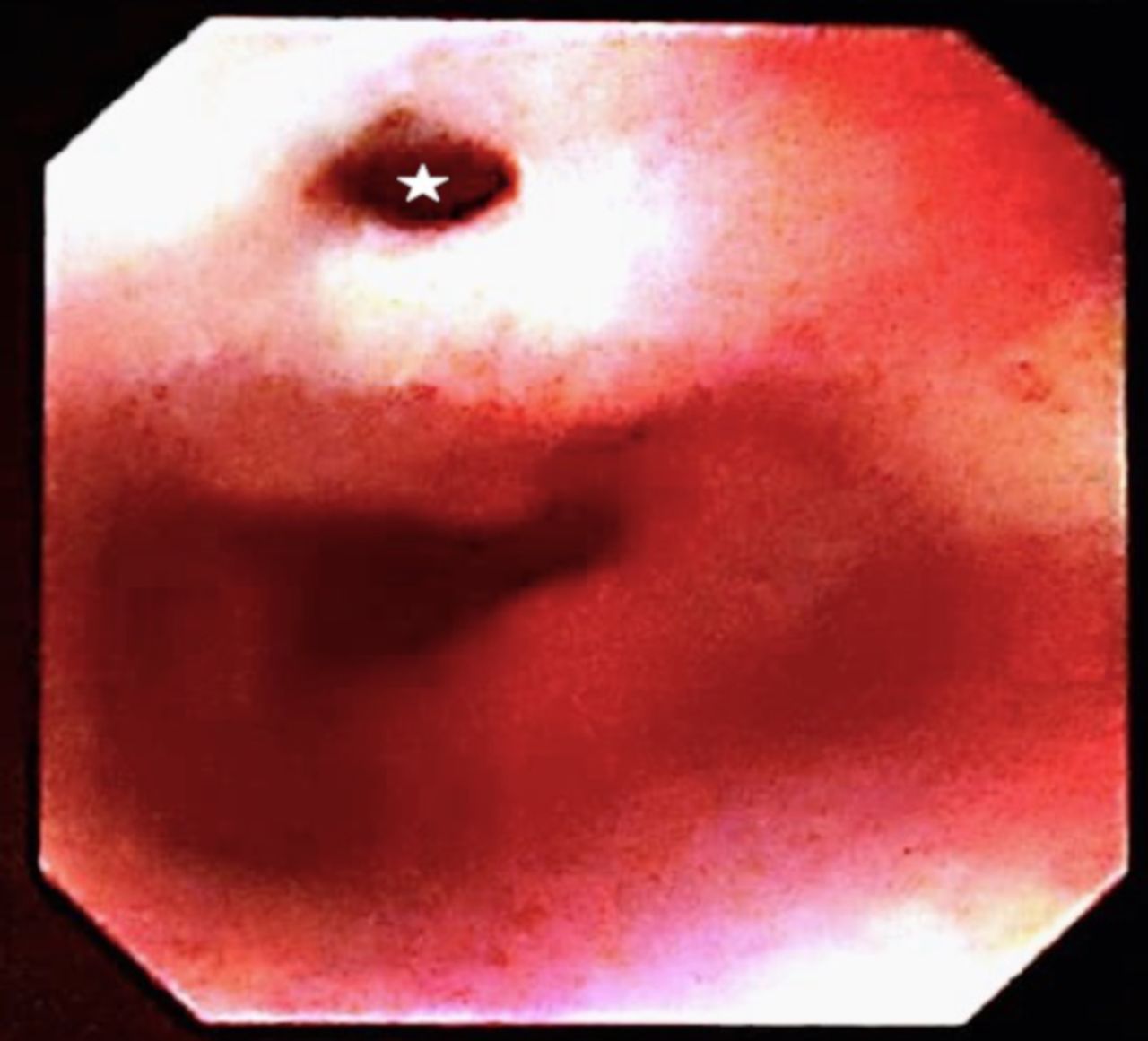
Subsequent bronchoscopy and oesophagogastroduodenoscopy (OGD) performed confirmed the presence of the tracheoesophageal fistula approximately 4 cm inferior to the level of the vocal cords (figure 1). Orogastric tube feeding was started to prevent further aspiration. Surgical repair of the fistula was later performed.

{kind=link}
Endoscopic photo taken during subsequent oesophageogastroduodenoscopy confirming the site of communication between the trachea and oesophagus (star).
The ‘H’ type is a rare form of tracheoesophageal fistulae with a prevalence of 4%.1 Early diagnosis of tracheoesophageal fistula is critical in guiding feeding, surgical repair and preventing further complications which include recurrent respiratory infections and death.
Although patients consistently experience coughing or choking episodes on feeding since birth and suffer from recurrent respiratory infections, diagnosis remains a challenge due to multiple factors. The fistulae are commonly small and inconsistently patent. The oblique configuration of the H-shaped tracheoesophageal fistula and close apposition of the trachea and oesophagus makes it difficult to appreciate radiologically. This may also be contributed to by the redundant nature of normal oesophageal mucosa which may transiently occlude the fistula.2
As a result, repeated radiological investigations using oesophagram studies may be required to make a definitive diagnosis.3 Special positioning and contrast delivery techniques have been described to aid in radiological diagnosis of this condition.2 In patients with typical symptoms with associated congenital anomalies such as the VACTREL sequence and chromosomal anomalies, a high degree of suspicion should be employed and timely bronchoscopy and/or OGD needs to be considered to exclude a tracheoesophageal fistula.
Although VFS studies are performed primarily to evaluate oral, pharyngeal and upper oesophageal swallowing function, our case report illustrates the importance of careful review of the images to ensure that uncommon diagnoses such as a tracheoesophageal fistula are not missed.
Learning points
A high degree of clinical suspicion to evaluate for tracheoesophageal fistulation should be employed in patients with feeding difficulties and recurrent respiratory infections with associated congenital anomalies.
H-type tracheoesophageal fistulae are rare, challenging to diagnose radiologically, and may require repeated investigations.
Although endoscopic evaluation remains the gold standard for diagnosis of tracheoesophageal fistulae, care on review of other imaging modalities (eg, video fluoroscopy swallowing) should be made to ensure uncommon diagnoses are not missed.
Footnotes
Contributors SYSL: contributed to conception, interpretation, drafting and revision of work. ESMH: contributed to conception, interpretation and final approval of work. The first author, SYSL, agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Parental/guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.