Article Text

Statistics from Altmetric.com
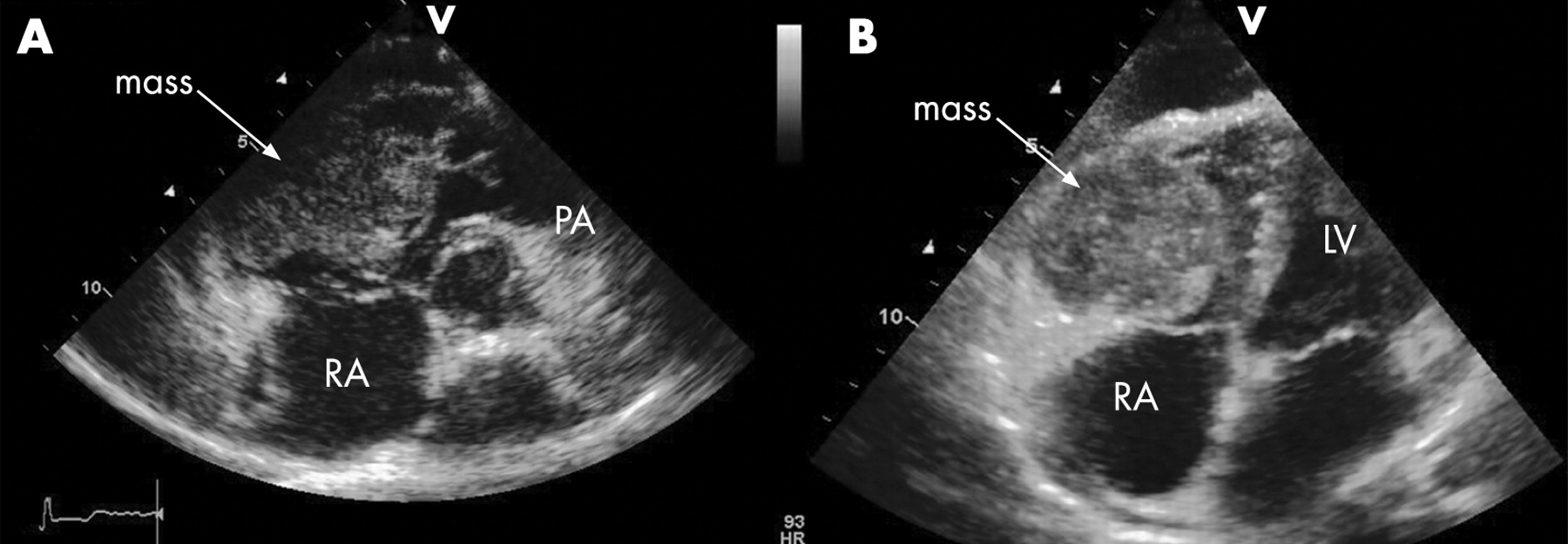
A 50-year-old woman presented with two syncopal episodes 7 months after resection of squamous cell carcinoma (SCC) of the base of the mouth. Investigation for metastatic disease at the time of diagnosis was negative. She had been immunosuppressed for 19 years with azathioprine and prednisolone after renal transplantation. A new loud ejection systolic murmur was noted in the pulmonary area.
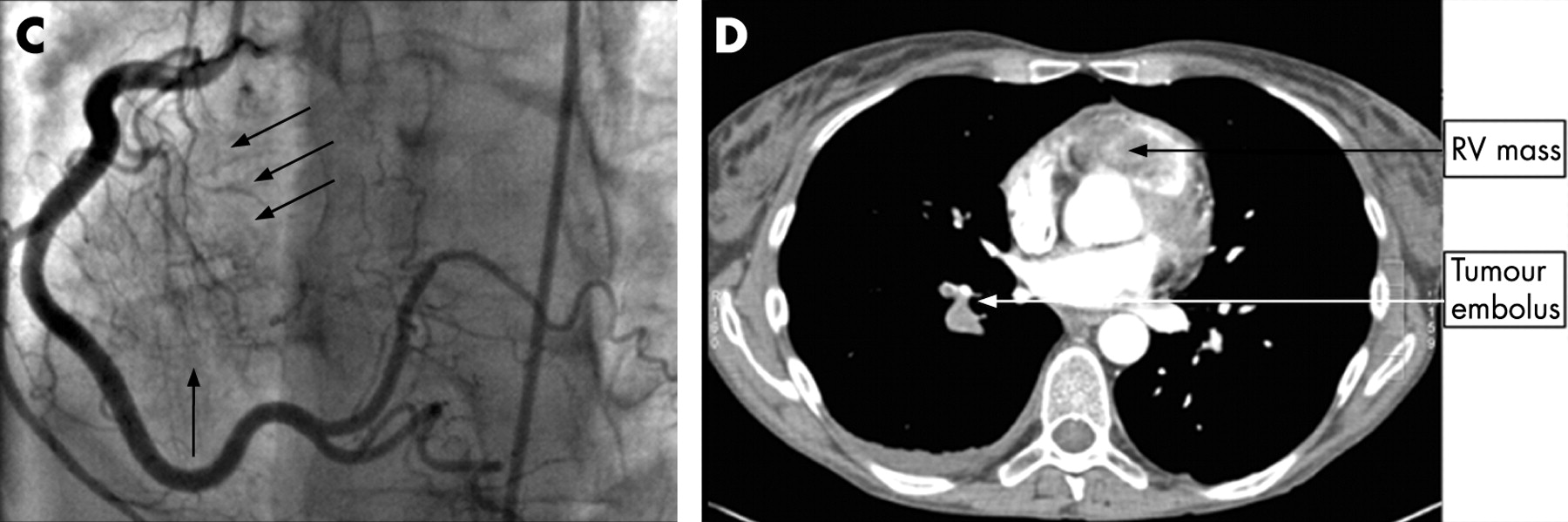
Transthoracic echocardiography showed a large mass (6×5 cm) attached to the right ventricular wall and extending into the main pulmonary artery, obliterating the right ventricular cavity (panels A and B). Coronary angiography showed neovascularisation from the right coronary artery (panels C). Computed tomographic scan of the chest showed the mass extensively involving the ventricular wall, as well as probable tumour emboli in the right pulmonary artery (panel D). Transvenous biopsy of the mass confirmed SCC. The patient started receiving radiotherapy, but died 6 days later.


{kind=link}
{kind=link}
Cardiac metastatic disease has been reported in up to 8% of patients who die from cancer, although it rarely results in clinical symptomatology. In particular, right ventricular outflow tract obstruction from SCC is extremely rare. We postulate that the patient’s immunosuppression may have contributed to aggressive tumour progression.
Acknowledgments
This article is reproduced with permission from Gurvitch R, Yan B P, Aggarwal A. Metastatic squamous cell carcinoma causing right ventricular outflow tract obstruction Heart 2007;93:697