Article Text

Statistics from Altmetric.com
A 37-year-old man presented with fever, abdominal discomfort and weight loss of 4 weeks duration. Examination revealed an ill-looking, emaciated patient with hepatosplenomegaly.
Complete blood counts, chest x ray, liver and renal function tests were normal.
Ultrasonography of the abdomen revealed multiple hypoechoic lesions in the spleen and liver. Computed tomography (CT) scan of the abdomen showed multiple, nodular, hypoechoic lesions in the spleen and liver, but no lymph node enlargement (fig 1). The possibilities of secondaries, lymphoma, tuberculosis and sarcoidosis were considered in view of the clinical and radiological findings.

Computed tomography (CT) scan of the abdomen showing splenic and hepatic lesions.
Chest CT scan, barium follow through, and upper and lower gastrointestinal endoscopies were normal, but endoscopic biopsies were not taken. Workup for tuberculosis, brucellosis and human immune deficiency syndrome were negative. CT guided biopsy of one of the hepatic lesions revealed necrotic hepatocytes. The patient left the hospital against medical advice to attend a traditional healer, but reported back with recurrent vomiting and severe abdominal pain. Oesophago-gastroduodenoscopy (OGD) revealed multiple ulcers in the stomach (figs 2 and 3), and biopsy revealed a gastric mucosa associated lymphoid tumour of B cell type (CD 20 positive). A bone marrow biopsy ruled out any infiltration and the patient was staged as stage IV-Bs.1 He was treated with chemotherapy and completed seven cycles of CHOO-R (cyclophosphamide, doxorubicin, vincristin, prednisolone, Rituximab).2 Follow-up OGD was normal except for mild erythema in the antrum (fig 4). An abdominal CT scan showed resolution of the hepatic and splenic lesions (fig 5) and the patient is now stable and in clinical remission.
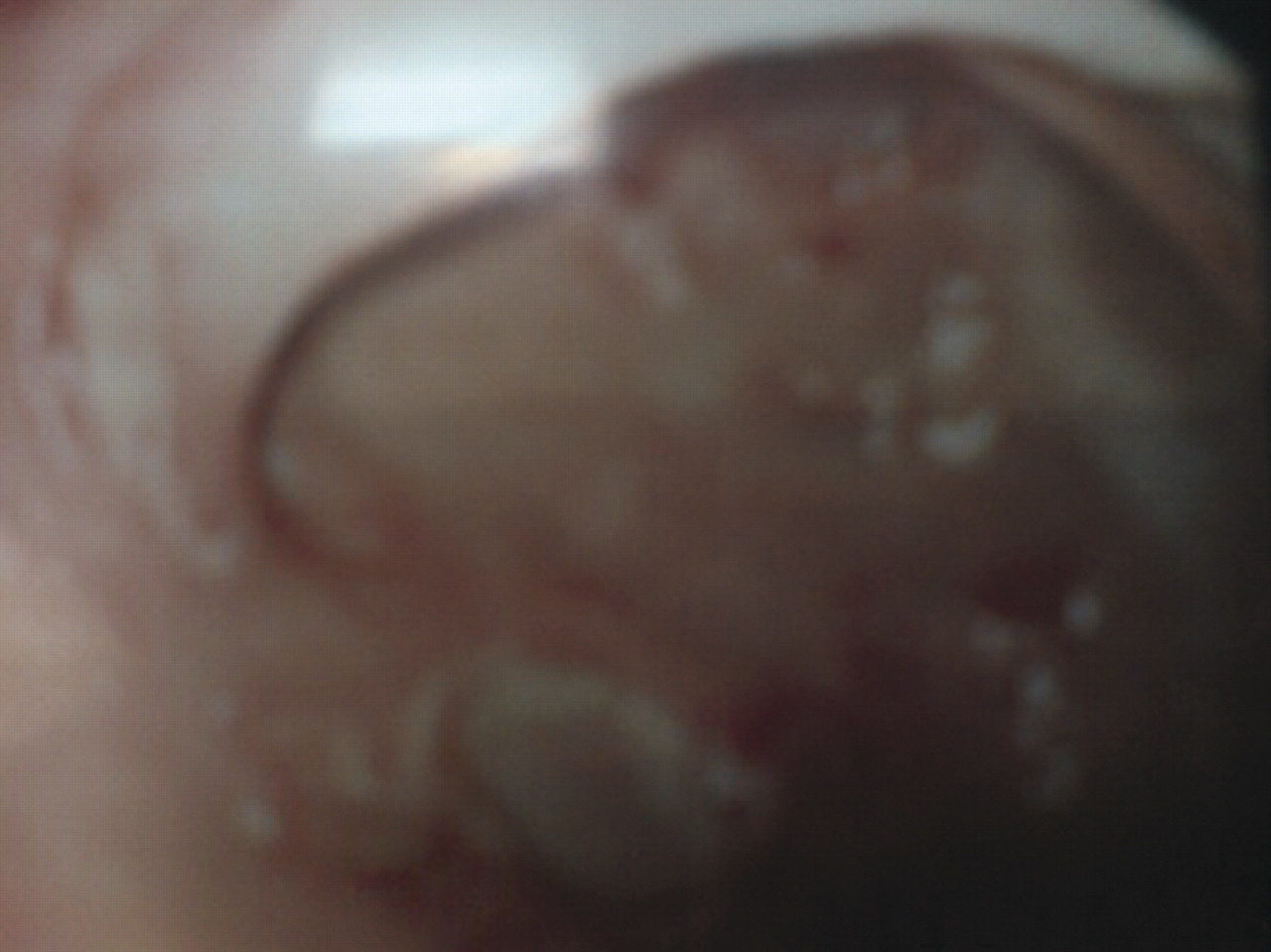
Extensive gastric ulcerations due to underlying lymphoma.

Endoscopy showing ulcerative lesions in the gastric antrum.

Endoscopic picture showing healed normal mucosa and mild erythema.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CT scan of the abdomen after treatment, showing resolution of most of the lesions.
From this case we conclude that gastric lymphoma can mimic benign conditions such as tuberculosis and sarcoidosis and malignant conditions with an unknown primary, especially when the presentation is unusual. In such situations a thorough workup of the upper and lower gastrointestinal tract is advocated, especially biopsies within biopsies (“well technique”) of gastric mucosa, to avoid any delays in reaching a diagnosis.
LEARNING POINTS
-
Endoscopic biopsies are indicated in cases with unusual presentation to avoid delay in reaching a diagnosis.
-
Differential diagnosis of lymphoma to be considered when appropriate radiological findings are noted.
-
Gastric lymphoma can spread to extra nodal sites such as spleen and liver without involvement of regional nodes and bone marrow.
-
In spite of disseminated disease, treatment options must be considered due to the favourable outcome achieved in this case.
Acknowledgments
We acknowledge the contribution of Wajiah Anjum of medical records.
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication