Article Text

Summary
We report a case where a patient slipped from the operating table during positioning for a laparoscopic colectomy. This occurred due to failure of the Velcro holding the mattress to the operating table. On further inspection, although the amount of Velcro was satisfactory to hold the patient, it had failed due to a combination of its poor positioning, table design and the build up of ‘fluff’ on the Velcro from the use of incorrect cleaning products. The episode was reported as a critical incident and review lead to the implementation of changes across theatres to prevent such an episode happening again.
Statistics from Altmetric.com
Background
-
Important safety issues
-
Clinical governance
-
Learning from errors.
Case presentation
We would like to report a near miss, involving a patient who slipped 50 cm down the operating table before being caught by the anaesthetist.
Over recent years our hospital has seen a shift towards increasing laparoscopic surgery, the hazards of which are well known to both surgeons and anaesthetists.1 To assist laparoscopic surgery the patient is subjected to some extreme positioning which carries additional hazards.2
An elderly overweight ASA 1 patient was scheduled for an elective laparoscopic sigmoid colectomy. This necessitates the Lloyd-Davies position with 30° head down and 10° of lateral tilt. The operating table we use (Maquet) has a mattress held onto the table by Velcro. Our departments’ usual practice is to place a long gel sheet on top of this mattress, rolled up at the head end on which the patient lies. This prevents the patient sliding down the mattress and off the table. We have stopped using shoulder supports due to the concerns over brachial plexus injury.
Following an uneventful general anaesthetic the patient was placed onto the operating table. After draping and establishment of adequate pneumoperitoneum the surgeon asked for head down positioning. During movement of the table the patient and mattress slid together on the table and had to be physically prevented from sliding onto the floor. On levelling the table and de-draping it was found that the Velcro holding the mattress to the table had failed.
Velcro was invented in 1941 by George de Mestral and initially used in the clothing industry. However, its versatility quickly led its widespread use.
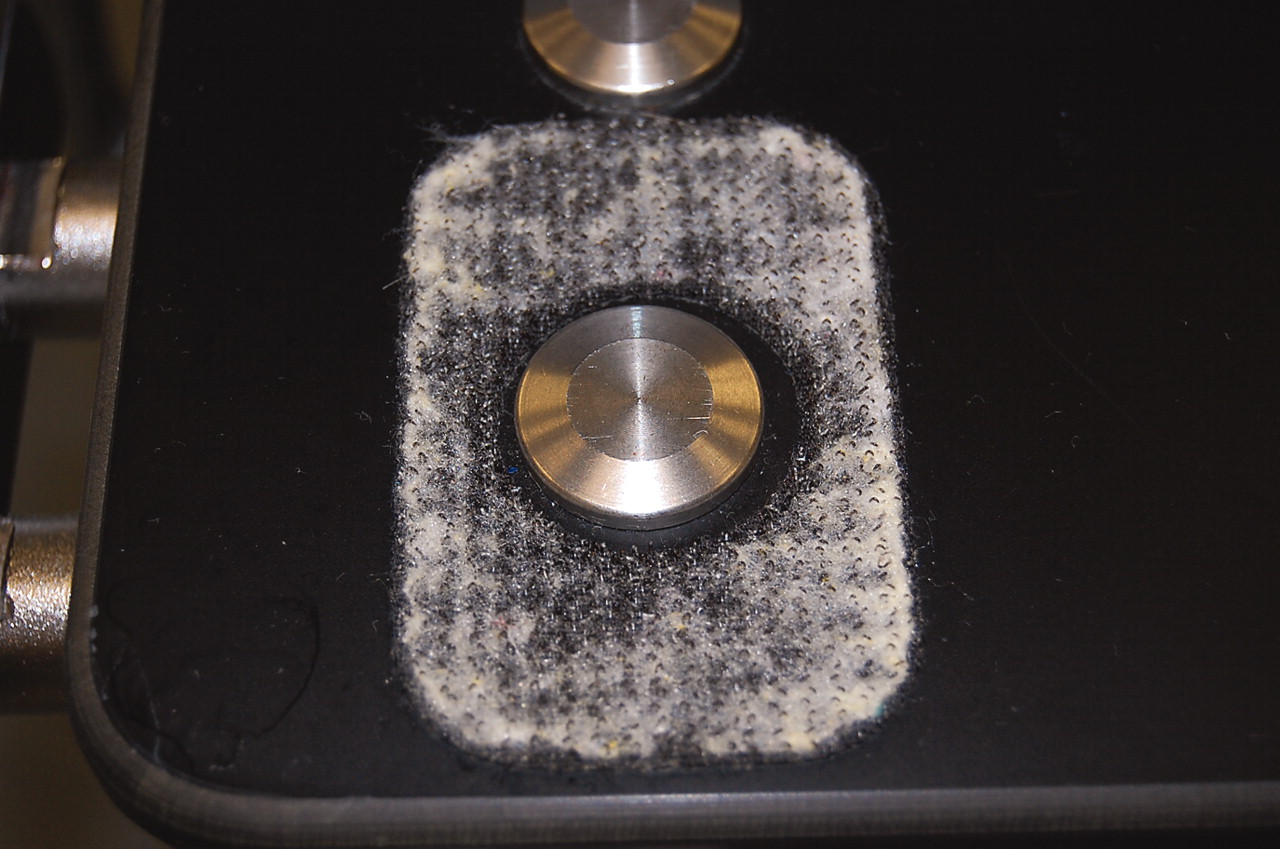
The amount of Velcro used to hold the mattress onto the operating table was many times more than needed to hold the weight of the patient; however, a combination of factors contributed to its failure in this case. First, there was a build up of cleaning fibres (lint or ‘fluff’) on the Velcro due to the use of inappropriate cleaning materials (fig 1). Secondly, the use of both the Perspex arm restraints and the endotracheal tube support placed between the mattress and the table had caused a partial separation of the Velcro. Thirdly, metal supports from beneath the table had been cut into some of the Velcro patches reducing their efficiency (fig 1). These supports also sat slightly proud and as such also contributed to the separation of the Velcro surfaces.

{kind=link}
A metal table support cut into a Velcro patch clogged with cleaning fibres.
Following a review of this critical incident the following changes have been made.
Maquet have replaced the old Velcro and attached additional strips of Velcro. They have not, however, recommended a minimum surface area of Velcro to prevent slipping.
Anatomically shaped shoulder supports have been reinstated with padding that reduces the possibility of brachial plexus injury. When using steep Trendelenburg positioning the Perspex arm restraints and tube support are not used. We have identified appropriate cleaning materials for use on the table to prevent clogging of the Velcro, and we are all more vigilant of the potential for slippage.
Outcome and follow-up
Changes in practice have been introduced across the anaesthetic department to prevent reoccurrence of such an event.
Discussion
After conducting a search on Medline, it appears that no similar cases have been reported. This case demonstrates that there are not just physiological dangers to extreme patient positioning. The anaesthetist must be aware of such dangers and be vigilant to their possibilities.
Learning points
-
Always check equipment, even if it is not considered as part of the ‘core’ anaesthetic equipment.
-
Be aware of the whole theatre environment.
-
Be aware that the use of equipment in a way it is not strictly designed for may lead to problems occurring.
Footnotes
Competing interests: None.
Patient consent: Patient not involved in a clinical trial