Article Text

Statistics from Altmetric.com
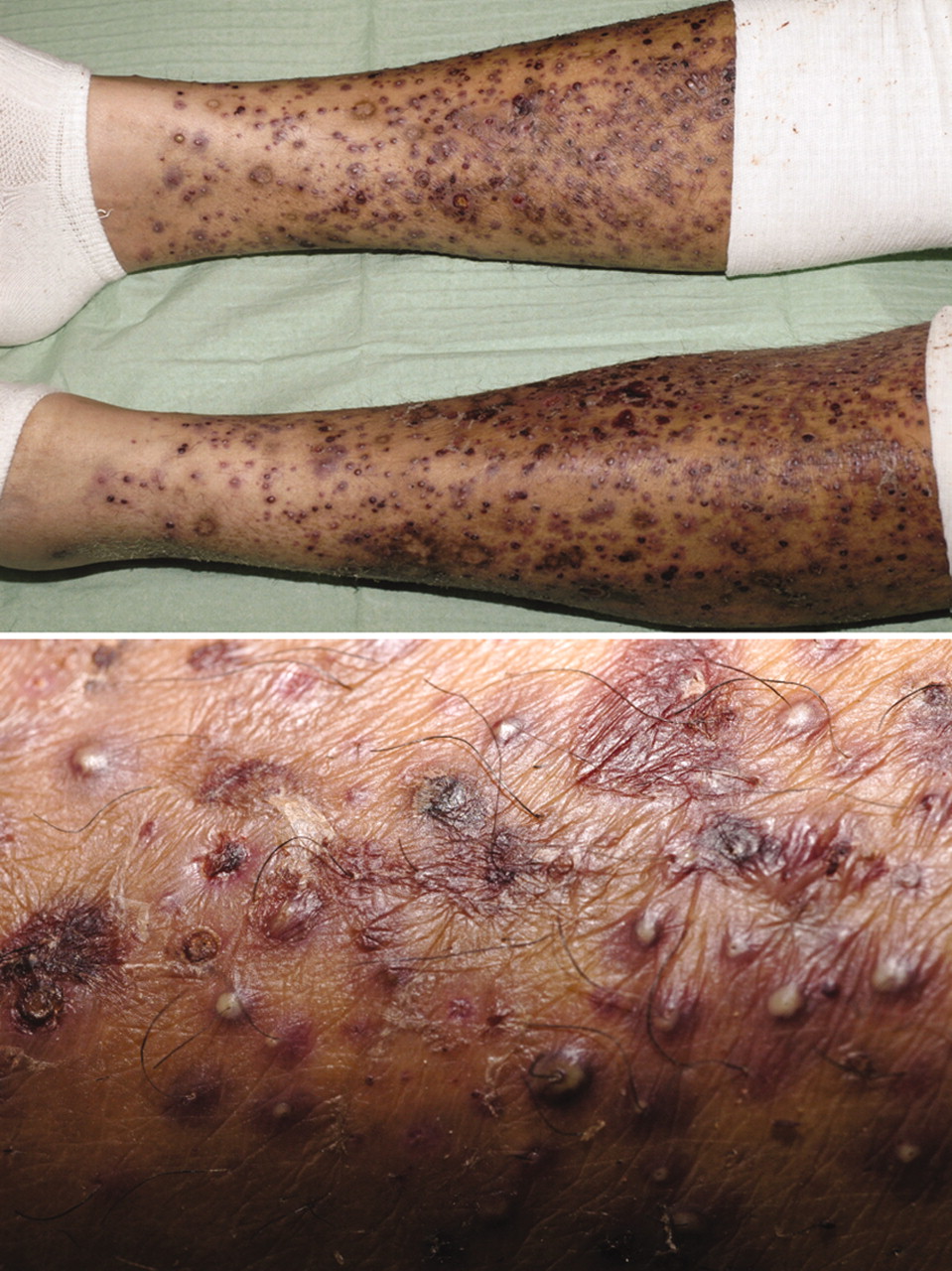
A 35-year-old British Asian, non-smoker, with non-small cell lung cancer was treated with erlotinib and had a good response despite having early widespread metastases in his lung, liver, skin, skeleton and thyroid. The size of his lung mass decreased within 2 months of starting erlotinib at 150 mg daily (fig 1), and the response was maintained for a further 8 months. He also developed the classical papulo-pustular drug rash, which is commonly seen with similar biological agents (epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors). Worsening of his now diffuse pustular drug eruption (fig 2) compelled us to discontinue his erlotinib. The rash was treated with steroids and erlotinib was re-started soon at a reduced daily dose of 100 mg, which was well tolerated. Subsequently, he relapsed with brain metastases with no evidence of disease progression at other sites. After palliative whole brain radiotherapy, erlotinib was continued and the patient was stable for a further 9 months. He died quite suddenly in April 2007.

{kind=link}
{kind=link}
LEARNING POINTS
Unlike chemotherapy, erlotinib is well tolerated.
Drug rash from erlotinib is easily treatable with steroids, minocycline, etc, and the therapy can usually be re-instituted.
Drug rash, although alarming, has a positive correlation with clinical outcomes such as disease response and overall survival1 and may be used as surrogate marker of treatment outcome. Contrary to the usual reaction when dealing with a drug rash, continuing the treatment using the offending drug is desirable.
REFERENCE
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication