Article Text

Statistics from Altmetric.com
A pregnant 28-year-old woman presented in the 34th week of gestation for a disproportionate increase in her abdominal size as compared to her previous pregnancy. The patient’s antenatal check-up was regular and routine antenatal screening for hepatitis and toxoplasmosis, rubella, cytomegalovirus and herpes (TORCH) were negative. There was no Rh/ABO blood type incompatibility. The patient denied any febrile illness in the past 8 months. Examination revealed a distended abdomen with multiple fetal parts and ultrasonography confirmed a twin pregnancy, with one of the fetuses having marked ascites (fig 1) with radiological features of meconium peritonitis. The patient was hospitalised and a paediatric surgeon was informed. After induction of labour, twins of gestational age 34 weeks were delivered.

Prenatal ultrasound showing fetal ascites.
Fetus 1 was a normal boy, weight 2 kg. Fetus 2 was a boy weighing 3 kg; he was lethargic and hypotonic. Abdominal examination revealed a massively distended abdomen (fig 2) with evidence of free fluid. Complete blood counts revealed white blood cells (WBC)=75 000, haemoglobin (Hb)=15.5 gm/dl, platelets=305 000. Blood gases (before/after mechanical ventilation) were partial (P)H=6.9/7.28, PCO2=100/45, PO2=60/70, HCO3=15.8/20, O2 saturation=71/96. Chest and abdominal plain x ray showed an elevated diaphragm and hazy abdomen (fig 3). Abdominal paracentesis showed a yellowish, turbid fluid with total cells 1080, monocytes 100 and on culture no growth. On laprotomy, a large amount of yellowish fluid flecked with white fibrinous material was removed from the abdomen. This same fibrinous material was distributed widely over the large and small bowels and the liver. A gangrenous portion of the end of small bowel was adherent to the liver and lateral abdominal wall. All adhesions were released and the perforated gangrenous part resected, and end to end anastomosis performed about 30 cm away from the ileocecal valve (figs 4 and 5) with preliminary T tube insertion. The distal bowel was of small calibre and full with pellets of meconium, which were washed out. Ventilator support and intensive care was given for 4 days and the baby passed stool on the 6th postoperative day. Then, feeding was started gradually. A contrast study after 12 days through the T tube revealed a normal bowel configuration (fig 6). The baby was discharged on full oral feeding on the 14th day. A sweat chloride test for cystic fibrosis was negative. On follow-up, the patient is doing well and gaining weight.

Baby after birth showing marked abdominal distension.

x Ray of the abdomen after birth showing hazy abdomen.
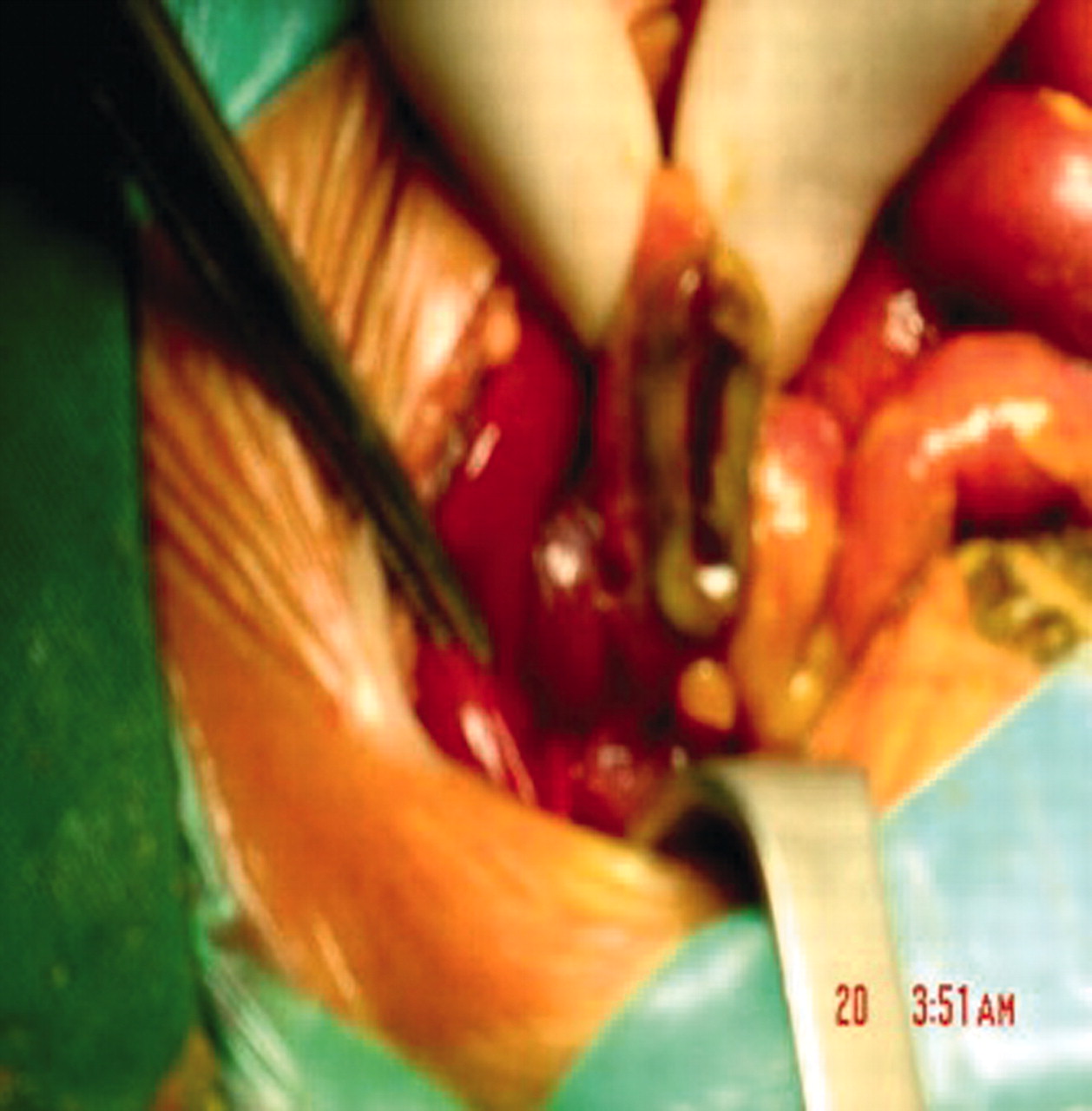
Intraoperative findings of ileal atraesia.
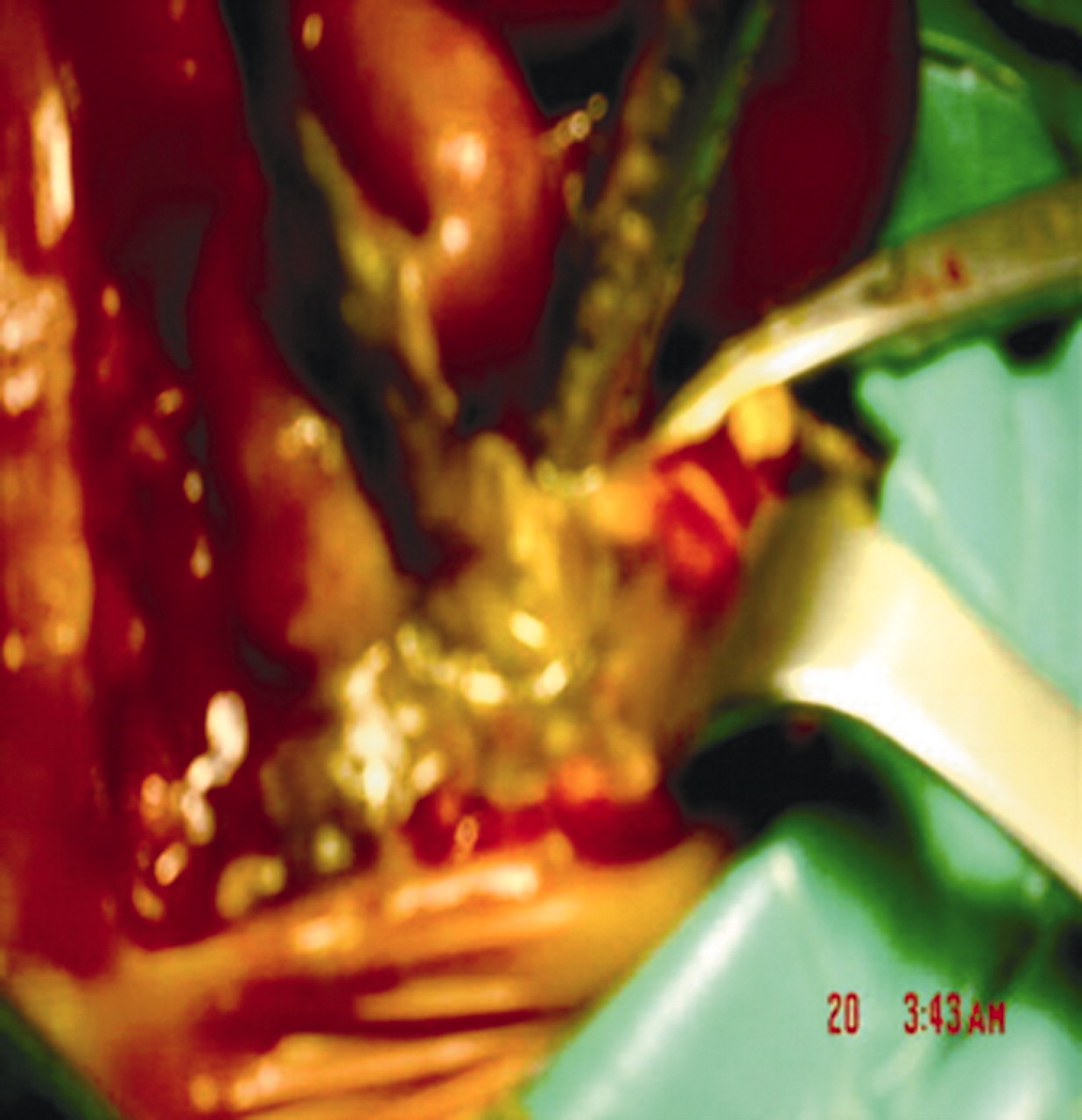
Intraoperative findings of ileal atraesia.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Postoperative contrast study delineating bowel configuration.
Meconium peritonitis (MP) is a sterile chemical peritonitis resulting from a small bowel perforation in utero1 that can be due to a number of causes (table 1).
Causes of in utero gut perforation and meconium peritonitis (MP)
Meconium peritonitis is classified into three groups as per antenatal ultrasonography findings: type I, large meconium ascites; type II, a large pseudocyst; type III, intra-abdominal calcifications, small meconium ascites and/or a shrinking pseudocyst.2,3 Our patient had type I meconium peritonitis. Some authors advocate a wait and watch policy as cases have resolved spontaneously, but others report high morbidity and mortality if timely intervention is not sought.2,4
With the advent of prenatal diagnosis the outcome for this condition has improved, especially the postoperative morbidity and mortality with survival rates up to 90%.5 In recognition of the fact that increased abdominal distension in utero can lead to hypoplasia of the lungs and increased neonatal respiratory distress and postoperative morbidity and mortality,1 we preferred earlier delivery and induction of labour; this has undoubtedly made immediate intervention possible, decreased morbidity and resulted in a shorter intensive care stay.
Acknowledgments
We acknowledge the contributions of Dr Ahmad Qadmani, Dr Ahmad Sidiqi and Dr Abu Mattar.
Footnotes
Competing interests: None.
Patient consent: Patient/guardian consent was obtained for publication.