Article Text

Statistics from Altmetric.com
An 85-year-old man was admitted to the Department of Orthopaedics with fever, polyarthralgia and back pain. Laboratory evaluation was notable for a C-reactive protein (CRP) level of 21.2 mg/dl (normal range, <0.3 mg/dl) and a leukocyte count of 13 400 cells/μl, however, no bacteria were detected in his blood culture. T2-weighted MRI of the lumbar spine revealed a high intensity in the L2–L3 disc (fig 1), and he was diagnosed as having suppurative spondylodiscitis and treated using antibiotics. However, his symptoms and serum CRP level (8.0 mg/dl) were not ameliorated, and the high intensity in the L2–L3 disc on lumbar spinal MRI still existed 2 weeks after the start of antibiotic therapy; he was then referred to our department. Symmetrical gallium-67 uptake in joints including shoulders and pelvic girdle on scintigraphy (fig 2), and elevated levels of serum matrix metalloproteinase 3 (136 ng/ml; normal range, 17.3–59.7 ng/ml) and vascular endothelial growth factor (1260 pg/ml; normal range, <115 pg/ml) as a synovial derived marker of inflammation suggested the presence of polymyalgia rheumatica (PMR).1,2 Gallium-67 uptake was also observed in the lumbar spine around L3, and gallium-67 uptake in the posterior image was more intense than that in the anterior image, suggesting the existence of spondylodiscitis. The patient’s clinical and biochemical characteristics showed a good agreement with the PMR diagnostic criteria.3 Corticosteroid therapy (20 mg/day) promptly ameliorated his symptoms and serum CRP (0.3 mg/dl at 10 days after corticosteroid therapy started), supporting the diagnosis of PMR.

T2-weighted MRI of the lumbar spine revealed a high intensity (arrow) in the L2–L3 disc.
{kind=link}
{kind=link}
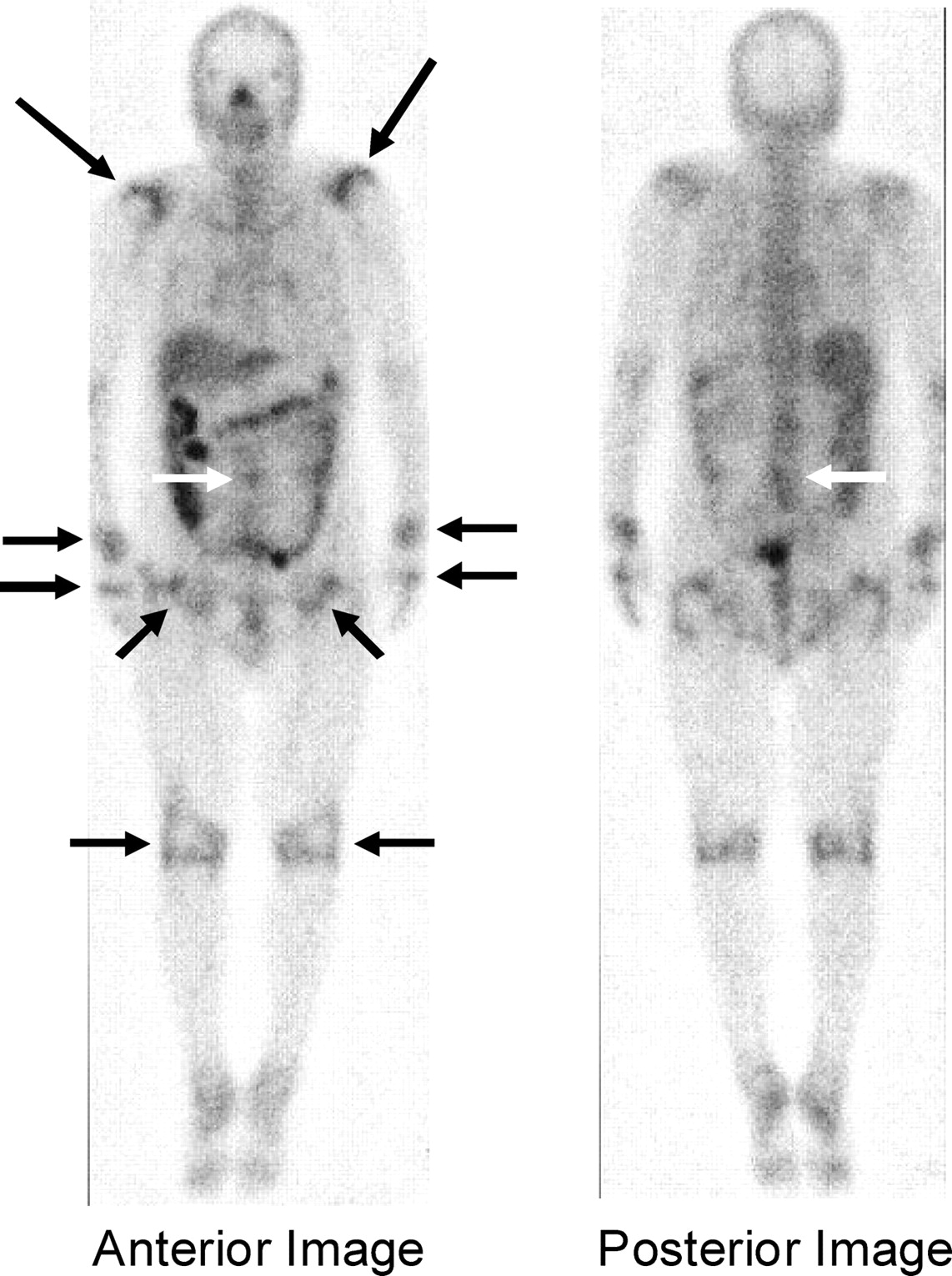
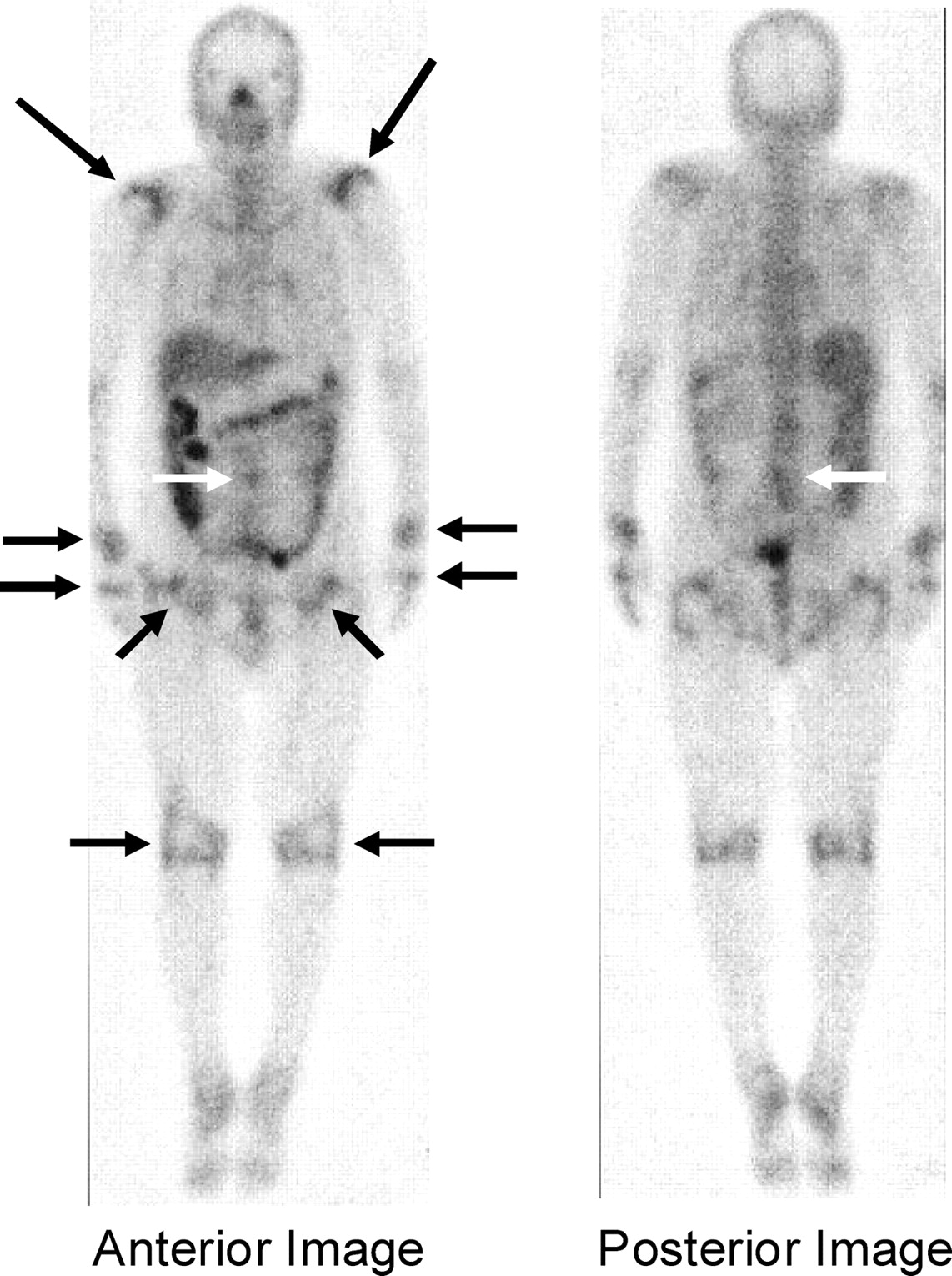
Symmetrical gallium-67 uptake in joints including shoulders and pelvic girdle on scintigraphy (black arrows); gallium-67 uptake (posterior–anterior) was also observed in the lumbar spine around L3 (white arrows).
LEARNING POINTS
-
This patient is the first case with polymyalgia rheumatica (PMR) who manifested aseptic spondylodiscitis.
-
PMR is occasionally accompanied with fever and an elevated serum C-reactive protein (CRP) level.
-
As this condition mimics infectious spondylodiscitis, it is important to recognise aseptic spondylodiscitis in PMR.
Footnotes
Competing interests: None.
Patient consent: Patient/guardian consent was obtained for publication.