Article Text

Statistics from Altmetric.com
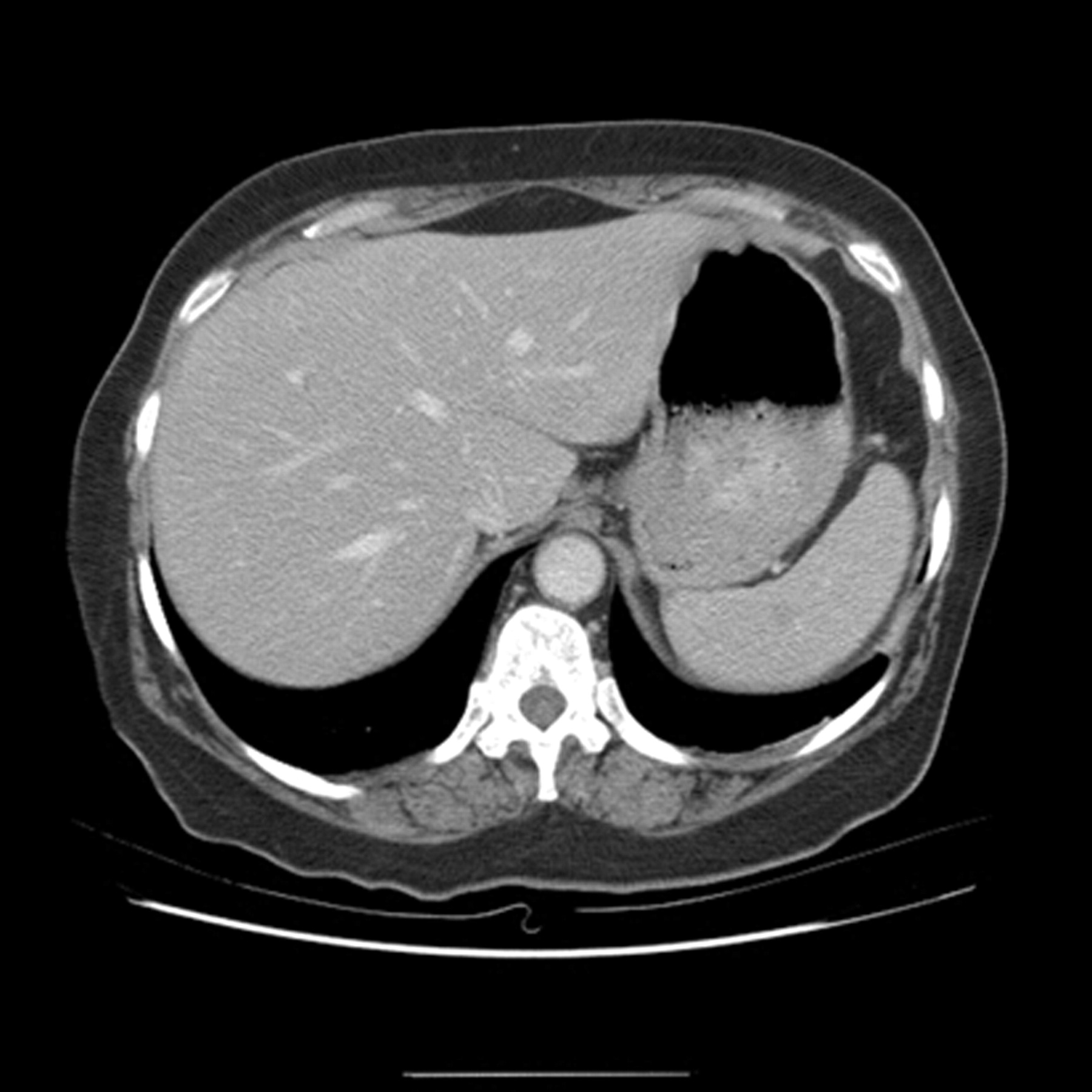
A 65-year-old woman presented with severe epigastric pain and vomiting. On examination she was pyrexial, tender with guarding in the epigastrium with associated leukocytosis and severely impaired renal function. She was given intravenous fluids and ciprofloxacin. A CT scan showed diffuse generalised thickening of the entire gastric wall (fig 1) with a presumptive diagnosis of gastric lymphoma.

CT demonstrating diffusely thickened wall of stomach.
Endoscopy showed diffuse gastric inflammation. Histology revealed marked submucosal inflammation and ulcer slough due to phlegmonous gastritis. She was treated with intravenous tazocin, teicoplanin and metronidazole for 10 days. Her symptoms and renal failure resolved. A repeat CT scan performed 3 weeks later showed a normal gastric wall (fig 2). Repeat endoscopy and histology confirmed normal gastric mucosa with no evidence of inflammation.

{kind=link}
{kind=link}
CT showing normal gastric wall.
Phlegmonous gastritis is a rare gastric infection caused by a variety of organisms, first described by Cruveilhier in 1820.1,2 Organisms include Streptococci, Enterobacter species and Escherichia coli.1,3 Diagnosis is difficult to make preoperatively and many of these patients end up with gastric resection due to severity of disease in the acute phase.2 Few cases have been successfully treated using antibiotics. Our patient made a rapid clinical, radiological and histological recovery in a short period of time. This case highlights the importance of considering the diagnosis of acute phlegmonous gastritis on observing a diffusely thickened gastric wall on CT. This should prompt endoscopy and biopsy for confirmation in the right clinical scenario. Once the diagnosis is made there is the potential for successful management using antibiotics and supportive therapy alone.
Footnotes
Competing interests: None.
Patient consent: Patient/guardian consent was obtained for publication.