Article Text

Statistics from Altmetric.com
Description
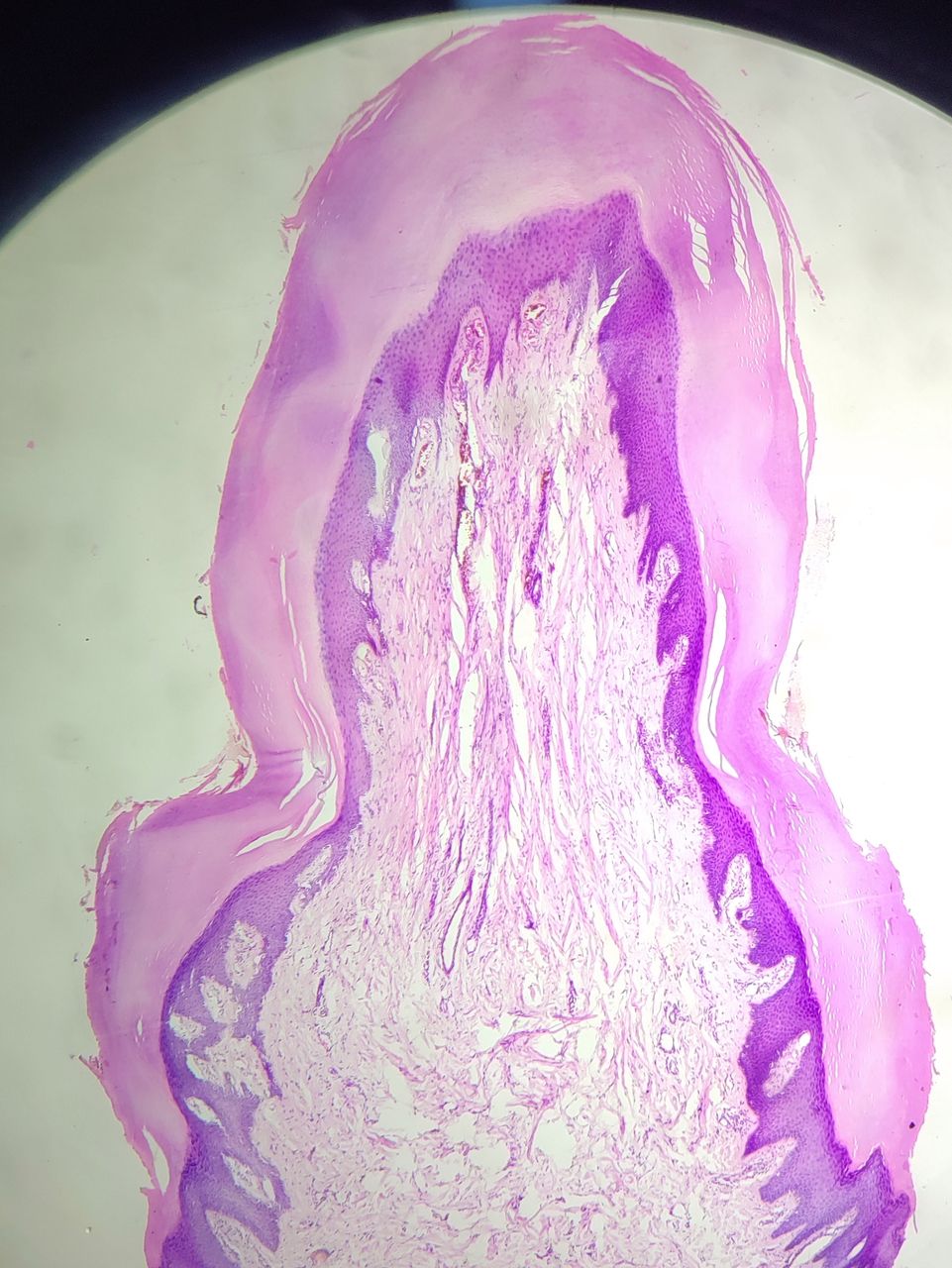
A man in his 50s presented to the dermatology outpatient department with a painless skin-coloured exophytic horn-like growth arising from the dorsal surface of the left index finger. It measured 3.5 cm in length with a broad base of 1.5 cm in diameter (figure 1). The growth had a characteristic hyperkeratotic collarette at its base. There was no history of any local factors like trauma or irritation. A clinical diagnosis of gaint acquired digital fibrokeratoma (GADFK) was made. Surgical excisional biopsy is performed as both a diagnostic and therapeutic procedure. Histopathology examination revealed a digitate lesion, composed of massive hyperkeratosis, acanthosis, a core of thick collagen bundles and vertically oriented small dermal blood vessels suggestive of ADFK (figure 2). Neural structures were absent and lacked adnexal structures, ruling out the possibility of the supernumerary digit. The final diagnosis of giant ADFK was confirmed because of the size of more than 1 cm and histology.

Horn-like growth arising from the dorsal surface of the left index finger with hyperkeratotic collarette at its base.

{kind=link}
{kind=link}
Hematoxylin and eosin stain reveals a digitate shaped, hyperkeratotic and acanthotic pedunculated lesion with peripheral collarette. The core is composed of dense collagen bundles, numerous capillaries and fibroblasts (original magnification, 5×).
ADFKs are benign, solitary, hyperkeratotic well-defined papules in digitate form looking like horns with a collarette of skin at its base. The lesions are usually dome-shaped, although they may present as elongated finger-like projections, as in the index case.1 2 Common sites of occurrence are on fingers and toes but can also be seen on the lower lip, nose, elbow, prepatellar area and periungual tissue. The size of the lesion is generally less than 1 cm, but there are reported cases of ADFK of more than 1 cm. These lesions are designated as GADFKs as in the index.2
The differential diagnosis of ADFK includes supernumerary digit, verrucae vulgaris, cutaneous horn, neurofibroma and pyogenic granuloma. Table 1 depicts the common conditions to be considered as differential diagnosis with their clinical characteristics and management.3–5
Differential diagnosis for ADFK
ADFK are usually asymptomatic but may be painful when traumatised. They are benign tumours with no risk of malignant transformation. They may affect the function of the digit and require removal. Surgical excision, cryotherapy, shave excision, curettage and cautery are all reported as treatment options. Excellent functional recovery with a satisfying cosmetic result is the expectation after complete surgical treatment. Usually, there is no recurrence.6
Classical collarette of skin at its base and specific histology helps in the diagnosis of ADFK.
Learning points
Classical clinical finding of collarette of skin at its base and specific histology helps in the diagnosis of acquired digital fibrokeratoma (ADFK).
ADFK is a benign tumour with no risk of malignant transformation.
Excellent functional recovery with a satisfying cosmetic result is the expectation after complete surgical treatment.
Ethics statements
Patient consent for publication
Footnotes
Contributors AI contributed for manuscript writing and SM for literature survey.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.