Article Text

Statistics from Altmetric.com
Description
The conventional median sternotomy approach in aortic and mitral valve surgery may increase injury risk in critically ill patients. Functional mitral regurgitation (MR) is frequently observed in patients undergoing aortic valve interventions. While aortic valve replacement (AVR) and transaortic Alfieri stich via right thoracotomy in these patients are technically challenged, this approach could reduce MR risk.1 Transaortic Alfieri stitch placement during AVR via median sternotomy is an additional feasible option to improve MR. This technique could potentially address mitral disease during AVR without left atriotomy requirement for mitral exposure. We have adopted a technique, in which an Alfieri stitch was placed in the mitral valve by aortotomy via right thoracotomy during endoscopic AVR.2–4
A woman in her 70s presented with progressive dyspnoea, a New York Heart Association Functional Class III, and moderate frailty (clinical frailty scale 7). Transthoracic echocardiography revealed severe aortic valve regurgitation and severe ventricular functional MR (figure 1).

Transthoracic echocardiography. (A) Transthoracic echocardiography revealed severe aortic valve regurgitation. (B) Transthoracic echocardiography revealed severe ventricular functional mitral valve regurgitation.
Considering her general condition, we decided to perform transaortic Alfieri stitch via right thoracotomy during endoscopic AVR.
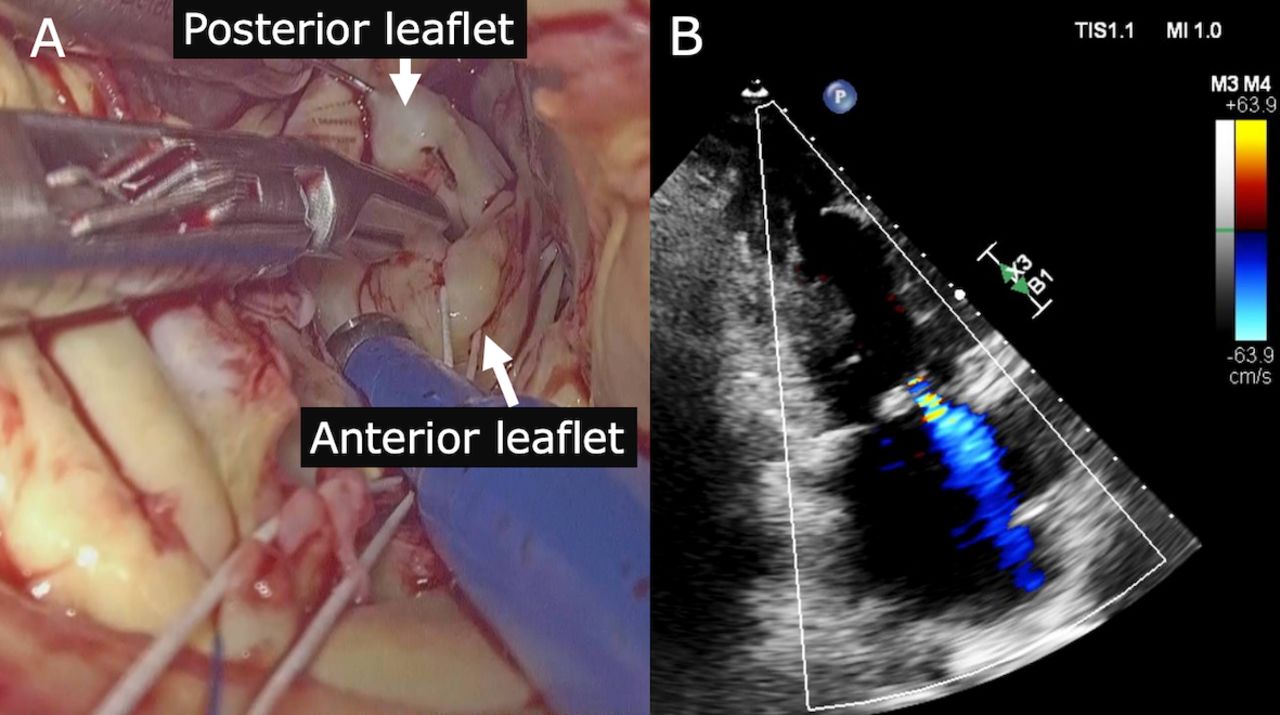
The aortic valve was exposed through an oblique aortotomy extending into the non-coronary sinus of Valsalva. Following aortic valve resection, mitral valve was clearly visualised by endoscopy through the aortotomy (figure 2A, video 1). The midpoint (equidistant from the two commissures) of the free edge of the anterior leaflet was identified. By lifting this area with a retractor, the posterior leaflet was exposed. Its midpoint was also lifted with a retractor. Identification of the midpoints is aided by observation of how the chordae fan out from both leaflets to the anterolateral and posteromedial papillary muscles. The midpoints of the posterior and anterior leaflets were then sutured together using a Gore-Tex CV-4 suture (W. L. Gore & Associates, USA). The suture was placed approximately 4 mm from the free edge of the leaflets. The existing aortic prosthetic valve was replaced with a 23 mm bioprosthetic valve (Carpentier-Edwards pericardial bioprosthesis; Edwards Lifesciences, Irvine, California, USA).

{kind=link}
{kind=link}
(A) Video: Endoscopic surgical findings of a mitral valve clearly visualised by aortotomy. (B) Postoperative transthoracic echocardiography revealed a mild-to-moderate ventricular functional mitral valve regurgitation.
Before discharge, postoperative transthoracic echocardiography revealed a mild-to-moderate MR (figure 2B). The patient was discharged home 15 days after surgery. Postoperative transthoracic echocardiography showed a mild-to-moderate MR and increased mean transmitral pressure gradient up to 1.85 mm Hg 6 months after surgery.
The described technique offers a simple way of correcting MR without adding significant time or complexity to the procedure. Although a mild-to-moderate MR with significant aortic stenosis usually improves after AVR, specific patient populations will benefit from a fast and simple repair. In retrospect, a repositioning of an Alfieri stitch might have been more efficient. This approach would be even more attractive for the Alfieri stitch, which is already both fast and simple per se. Therefore, the simplicity of the procedure might promote a more aggressive correction of concomitant MR, and consequently, eliminate late corrections of the residual MR. This innovative approach to MR is particularly valuable in technically challenging cases, such as reoperations and fragile patients.
Several technical concerns should be emphasised. The suture must be placed centrally at a point best identified by pulling the leaflet taught and identifying the decussation point of the chordae from the two papillary muscles on each leaflet. Since no paracommissural sutures are possible, only central MR can be addressed.
The endoscopic view is wider than direct vision through a limited wound and is less affected by the anatomical variations of the patients. To our best knowledge, this case represents the first report of endoscopic transaortic Alfieri stitch via right thoracotomy during AVR.
Learning points
We presented a case of endoscopic transaortic Alfieri stitch via a right thoracotomy during aortic valve replacement (AVR).
Endoscopic transaortic Alfieri stitch via a right thoracotomy during AVR is safe and feasible, with potentially improved surgical view.
This innovative approach to mitral regurgitation is particularly valuable in technically challenging cases, such as reoperations and fragile patients.
Ethics statements
Patient consent for publication
Footnotes
Contributors MS: Critical revision of the article, writing, editing and data collection. YM: Contributed to original drafting, the design and implementation of the research and data collection. AY: Finalised the manuscript. KG: Finalised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.