Article Text

Statistics from Altmetric.com
Description
Dermatofibrosarcoma protuberans (DFSP) is a rare soft tissue tumour commonly affecting young adults. It is an intermediate-grade malignancy that rarely metastatizes, but has a high recurrence rate. Diagnosis is established by histopathology.1 Here, we describe a typical presentation of DFSP in a woman and the utility of dermoscopy and radiologic imaging in the diagnosis and management.
A woman in her 40s presented with an asymptomatic enlarging lesion on her right shoulder from past 1 year. Examination revealed a firm, non-tender, skin-coloured to brown multilobular plaque measuring about 1.5×1.5 cm (figure 1A). Polarised dermoscopy (using DermLite DL3, 3Gen, San Juan Capistrano, California, USA) from different areas of the lesion revealed white homogeneous structureless areas surrounded by linear serpentine and branching vessels (figure 1B), linear serpentine vessels on a pink background (figure 1C) and pigment network over a whitish background (figure 1D). The clinico-dermoscopic diagnosis of DFSP was confirmed by histopathology showing monomorphic spindle-shaped cells, without atypia or mitoses, diffusely infiltrating the dermis and subcutis in whorls or storiform pattern. Epidermis showed increased melanisation of basal layer (figure 2A). Immunohistochemistry was not performed due to lack of facilities. CT delineated a well-defined soft tissue attenuation mass extending into subcutaneous plane (figure 2B) and also confirmed absence of chest metastases (figure 2C). Based on the radiological delineation of the tumour, a wide excision with 2 cm margins was performed and the wound closed primarily. Intraoperative frozen sections and postoperative histological assessment revealed tumour-free resection margins. Regular follow-up (once in 3 months) was advised.
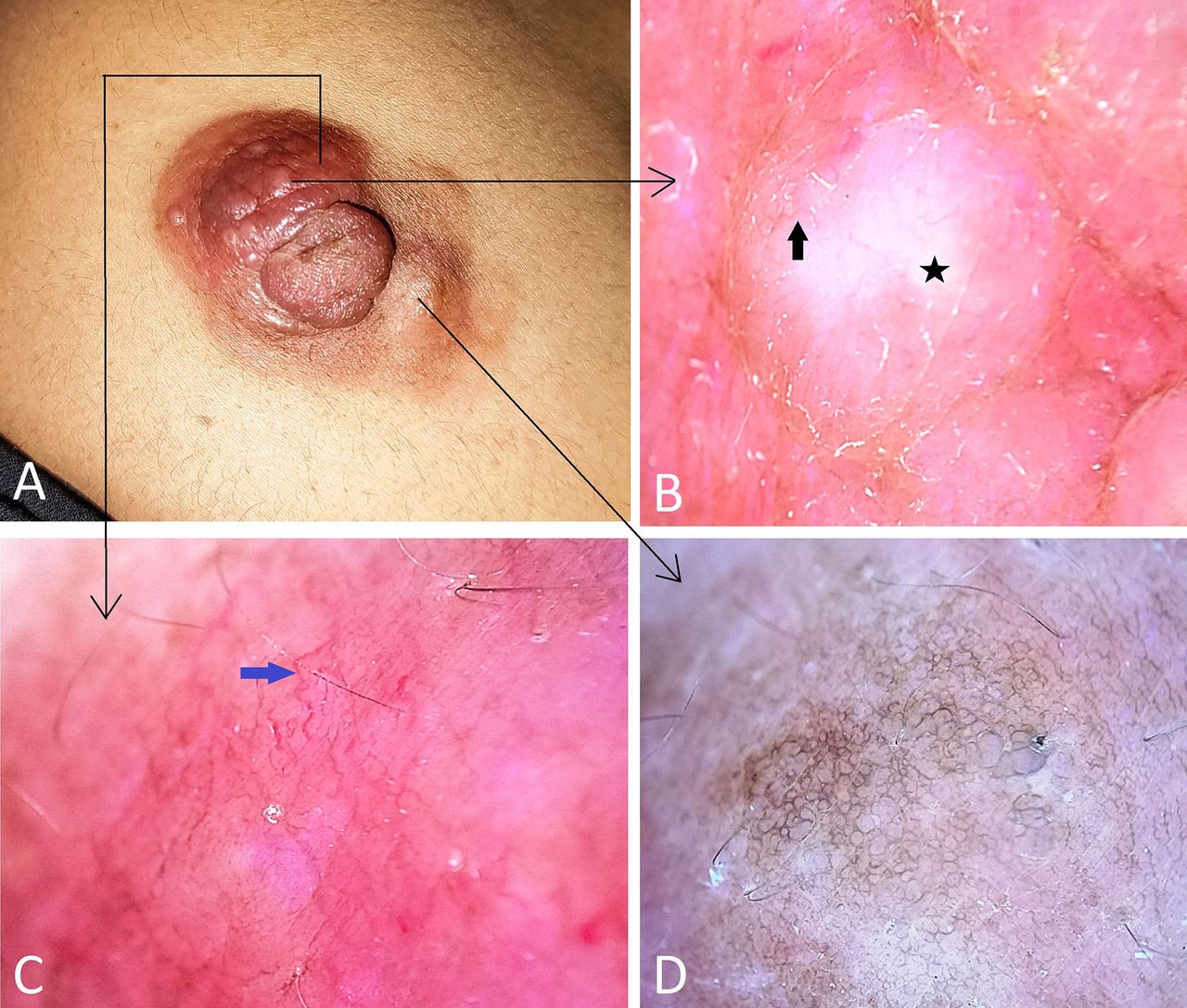
Skin-coloured to brown circumscribed plaque with multilobular surface (A). Dermoscopy from different areas of the lesion indicated by black slender arrows show white homogeneous structureless area (B, black star) surrounded by linear serpentine and branching vessels (B, black solid arrow), linear serpentine vessels on a pink background (C, blue arrow) and a delicate pigment network over a whitish background (D). (Polarised dermoscopy, ×10).

{kind=link}
{kind=link}
Photomicrograph (H&E, ×5) showing diffuse infiltration of uniform spindle-shaped cells in whorls and storiform pattern involving the dermis and subcutis (A) High-resolution CT showing a well-defined soft tissue attenuation mass extending into subcutaneous plane (B, white arrow), and normal lung fields (C).
The most common presentation of DFSP is that of a slow-growing firm-hard plaque with multinodular surface that initially resembles a keloid. The trunk, shoulders and pelvic region are frequently involved. Other forms include morphea-like, atrophoderma-like and angioma-like DFSP. Majority of the patients exhibit a t(17;22)(q22;q13) translocation predisposing tumour formation following trauma.1 2 Common dermoscopic features in DFSP include pink background, hypopigmented or depigmented areas, arborizing telangiectasia, linear vessels, shiny white structures and pigment network.3 We observed similar features. The homogeneous white areas correspond to diffuse fibroblast aggregates, telangiectasia to the dilated vessels and pigment network to the increased basal layer melanisation.
Microscopically, DFSP is a tumour localised to deep dermis and subcutis showing diffuse infiltration of monomorphic cells in whorled or storiform patterns. The cells show small oval or spindle-shaped nuclei with scanty cytoplasm and low mitotic rate. Immunohistochemically, majority show positivity with CD34 and negativity with FXIIIa, SMA, desmin, S100 and cytokeratins. Histological variants include a fibrosarcomatous type (showing high mitotic index and marked nuclear atypia) and a pigmented variant (Bednar tumour).1 2 4 On CT imaging, DFSP commonly shows well-defined isodense cutaneous or subcutaneous nodule without calcification. We noted similar features. MRI usually shows a well-defined isodense nodule compared with muscle on T1-weighted images, and on ultrasound, as a low echogenic mass with rich vascularity.5
Although metastasis and fibrosarcoma transformation are rare, being locally infiltrative, DFSP has a high postoperative relapse rate. Hence, the principal aim of surgery is to ensure clean tumour-free resection margins. Mohs micrographic surgery is hence considered ideal. Wide excision with at least 2 cm margin is recommended if the latter is not possible. For recurrent lesions requiring wide and deep resection and/or for facial lesions, ensuring complete excision to achieve tumour-free resection margins and achieving best possible aesthetic outcomes are necessary. In this regard, pedicled latissimus dorsi myocutaneous flap and anterolateral thigh perforator free flap reconstructions have been employed to good effect.6 7 Most of the recurrences after primary excision tend to occur within the first 3 years with a median of 32 months noted in a study.1 8 9 Hence, a quarterly to half-yearly follow-up during this period and a lifelong annual follow-up thereafter is recommended. Complete physical, cutaneous and systemic examination should be performed at each visit and robust evaluation done only when metastasis is suspected.1 8
Learning points
Dermatofibrosarcoma protuberans (DFSP) is a rare fibrohistiocytic tumour that is considered intermediate between benign dermatofibroma and malignant fibrosarcoma.
Although histologically exhibits banal features, DFSP is a locally infiltrative tumour accounting for its high recurrence rate following excision and can rarely metastatize.
Diagnosis of DFSP is established by histopathology. Dermoscopy and radiological assessment are useful non-invasive adjuncts to assert the clinical diagnosis. The latter also helps in delineating the tumour extent to facilitate optimal surgical resection and also in ruling out distant metastases.
Ethics statements
Patient consent for publication
Footnotes
Contributors KAA: data compilation, data analysis, manuscript preparation, manuscript review. ABP: data analysis, manuscript preparation, manuscript review. ALT: data compilation, data analysis, manuscript preparation, manuscript review. AI: data analysis, manuscript review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.