Article Text

Abstract
We report a newborn with neurocristic cutaneous hamartoma of the scalp. He was delivered at term via caesarean section due to a previous scar and presented at the neonatal unit on the fifth day with giant congenital nevi on the scalp and disseminated melanocytic nevi throughout the body. The MRI scan of the brain showed a defect at the occipital region with herniation of the occipital lobes and ventricles through the defect, with infratentorial brain parenchyma exhibiting normal signal return and intact cerebellum. The initial diagnosis was a giant haemangioma, which has ruptured, and possible cytomegalovirus infection, causing ‘blueberry muffin’ syndrome. On follow-up, the hamartoma/haemangioma-like mass regressed, and a large well-demarcated melanotic patch on scalp and large encephalocele were seen. This infant is now being scheduled for neurosurgical intervention.
- Hemangioma
- Neurology
- Skin cancer
- Congenital disorders
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Neurocristic cutaneous hamartoma (NCH) is a rare entity, with no standard recommendations for treatment. Non-recognition may lead to wrong diagnosis and management. Close follow-up is of the essence because of the risk of transformation into malignant melanoma over time.
Congenital NCH of the scalp is very rare and is presumably a result of aberrant development of neuromesenchyme, and has a great risk of transforming into malignant melanoma. It can occur in the neck, back or scalp with highest predilection for the scalp. Its clinical importance lies in the potential for misdiagnosis and capacity for malignant transformation over time.1 2
We report a case of NCH of the scalp, which to our knowledge, is the first in the unit.
Case presentation
A term neonatal boy born of non-consanguineous parents, with birth weight of 3.2 kg, was referred to our neonatal unit with a scalp swelling and disseminated black spots on his body since birth.
On examination, a well-defined fluctuant mass measuring 20×18 cm was noted, occupying the parieto-occipital area. The mass was bleeding profusely. There was overlapping of the sagittal suture, and loss of continuity of the parietal and occipital bone. A large hyperpigmented macule covered around 80% of the swelling (figure 1A,B), and disseminated hyperpigmented macules and nodules (melanocytic nevi) throughout the body, ranging from few millimetres to several centimetres in diameter (figure 2). There were no focal neurological deficits noted.

(A) Giant congenital nevi on scalp, with ulceration. (B) Nevi surrounded by hyperpigmented melanocytic macular patches (right).

Disseminated hyperpigmented macules and nodules, and melanocytic nevi, widespread at the back (left) and all over the lower limb (right).
The cardiac and renal functions were normal. The child was able to suck and had normal reflexes, but the vision was not tested.
The first impression of the lesions raised suspicion of cytomegalovirus infection; on close observation, it showed typical melanocytic nevi.
Investigations
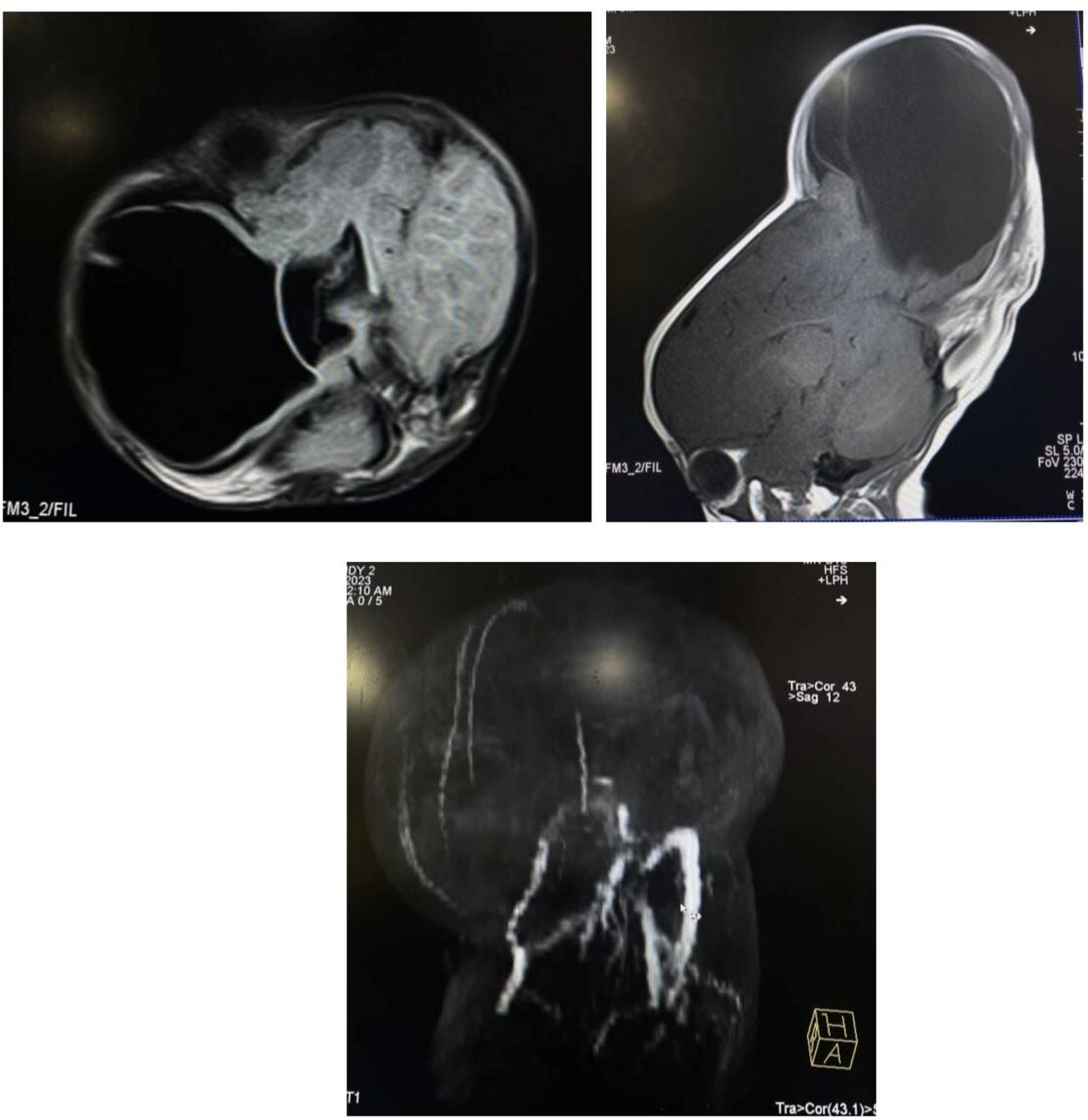
The initial MRI of the brain showed a defect in the occipital region associated with herniation of the occipital lobe and ventricles through the gap in the calvarium and cutaneous defect, more on the right side. Infratentorial brain parenchyma exhibited normal signal return. There was no intra-axial or extra-axial space-occupying lesion. The cisterns and sulci, brain stem, sella and suprasella region all appeared normal (figures 3 and 4).

MRI of the brain axial view showing a defect in the occipital region (left) associated with herniation of occipital lobe (right), more on the right side.
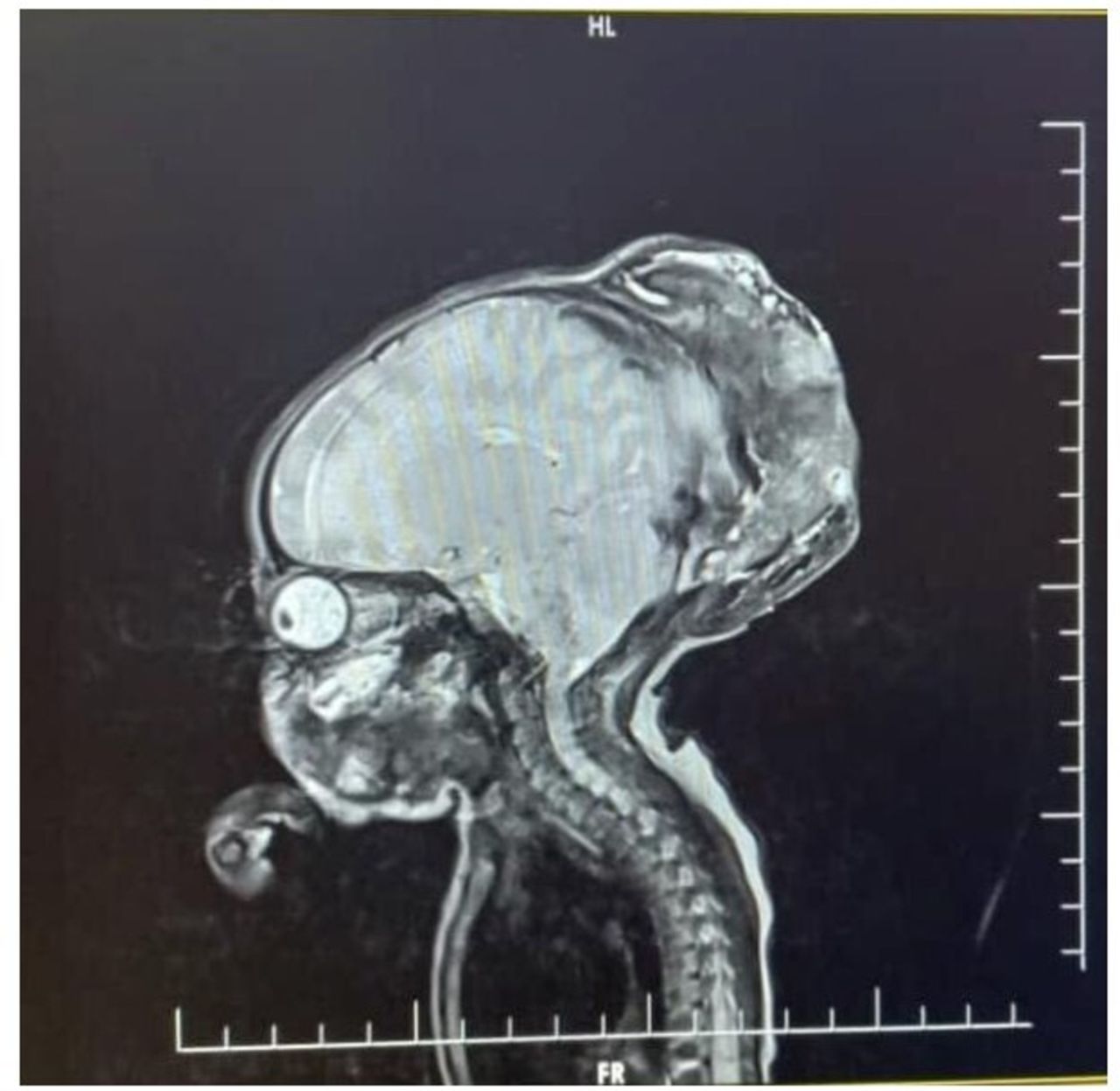
MRI of the brain, T1-contrasted sagittal view showing skin defect in the occipital region, with heterogeneous signal intensity within the scalp.
A biopsy of the swelling could not be attempted due to the risk of bleeding. Screening echocardiography showed a structurally normal heart. Based on the ultrasound of the abdomen, there were no abnormalities of the liver, spleen, kidneys and intestines. Serum IgG and IgM for rubella and cytomegalovirus infection were negative.
Differential diagnosis
The differential diagnosis was neurocutaneous melanosis. The baby however did not have any neurological deficits, and no obvious melanocytic nevi were noted in the brain.
Treatment
There is no standard recommendation for treatment of NCH. The hamartoma on the scalp was dressed daily and blood transfusion was given. The bleeding was controlled, and the swelling regressed significantly. The herniation of brain and excision of the hamartoma have not been done, for fear of bleeding and the extent of the hamartoma. For the haemangioma-like swelling, propranolol was given for 5 weeks. Although wide local excision is ideal, this was not possible due to the size of the mass and risk of bleeding.
At infancy, after regular dressing and propranolol, there was regression of the mass and healing with granulation tissue as seen in figure 5.

Hamartoma of the scalp after 3 weeks of daily dressing and propranolol.
Outcome and follow-up
The baby is still being followed up and the mother has been counselled. He is being seen at the neurosurgery clinic on a weekly basis.
The therapy with propranolol was effective; the haemangioma-like swelling regressed, but the encephalocele, which was small, grew bigger because of the enlargement of the ventricles. A repeat MRI of the brain 6 weeks later shows that the extension of the occipital encephalocele has enlarged. The current size of the encephalocele is about 18×18 cm and the cavity is filled with ventricular fluid. The child is scheduled for a neurosurgery this week for a shunt to reduce the size of the encephalocele.
The diagnosis of neurocristic syndrome is still high on the list because of multiple melanotic patches all over the body and the encephalocele. Neurocristic syndrome is associated with neural tube defects.3
We have referred the baby to the neurosurgeons and haemato-oncologists. The neurosurgeons are planning to insert a shunt to reduce the size of the obstructed ventricles in the encephalocele. The haemato-oncologists are asking us to keep a clinical eye of the melanotic patches for any changes clinically. The mother has refused for a skin biopsy.
Figure 6 shows a giant melanotic patch on the scalp. The haemangioma has regressed and there is the encephalocele, which is now more prominent.

Images of large melanotic patch and scar, and a well-demarcated encephalocele.
Figure 7 shows the MRI showing that the haemangioma-like mass has now resolved and the current MRI shows a well-demarcated encephalocele.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
MRI showing that the haemangioma-like mass has now resolved and the current MRI shows a well-demarcated encephalocele.
The child has been failing to thrive.
Discussion
NCH of the scalp is a rare lesion, presumably resulting from aberrant development of neuromesenchyme. Its elements reflect the spectrum of differentiation inherent in neural crest-derived cells.4 It is most observed in the scalp and can be congenital or acquired.5 It was first described by Tuthill et al as pilar neurocristic hamartoma.6 No genetic disposition has been observed.4
NCH consists of a combination of elements histologically, including nevomelanocytes, pigmented dendritic cells, Schwann cells, spindle cells and fibroblasts thus underscoring the pluripotent nature of neural crest cells.1 2 4 7 8 NCH stain positivity for S-100, CD57, HMB-45, Melan A, collagen 4 and CD34.8 The surrounding stroma in NCHs, as well as the areas with schwannian differentiation, shows increased CD34-positive cells.
A significant number of NCHs have acquired a malignant melanocytic component,1 2 which could not be ascertained in this stage with our tumour due to the failure to proceed with a biopsy.
Turel et al described a female infant who had a right occipital scalp swelling since birth.9 There were no focal neurological deficits as was seen in our case, and the mass occupied the right parieto-occipital scalp. A biopsy attempt was done but terminated due to excessive bleeding. In Turel et al’s report, a total excision of the mass was done.
Diagnosis can be a challenge as few cases have been reported, and if these lesions display a prominent melanocytic component, they can be difficult to differentiate from other pigmented cutaneous abnormalities, such as congenital nevi, as there can be some histological overlap.4 10
No specific guidelines exist for managing these patients. Emphasis is put on long-term follow-up with cancer surveillance, which is ongoing in our case, with close monitoring for malignant transformation.2 11
This is a rare case of neurocristic syndrome, and the haemangioma responded well to propranolol. There are very scarce reports of such conditions that we report here. This infant has multiple melanoses and large scalp melanotic patches, which are associated with encephalocele. Neurocutaneous melanoses are common in giant melanosis and about 12% develop this, as seen in our infant. 3 12 13
Our case demonstrates the importance of early diagnosis, treatment and long-term follow-up. This may be a challenge in a resource-limited country like ours due to a lack of experts in all healthcare centres and financial constraint to return to clinic, which may lead to loss to follow-up.
Early recognition in the neonatal period and supportive treatment are important. The infant has been referred to the nutritional unit for better nutritional management.
Patient’s perspective
I was very scared when I first saw my baby. I immediately decided to come to the bigger hospital in the city so that he could be attended this national hospital despite not having enough funds.
It was a long trip, the swelling on the head was not bleeding when my baby was born, but by the time we reached the city it started to bleed. I have had great support since I arrived here. The team of doctors and nurses have been nice, my baby was immediately investigated, and they dressed the wound daily. One doctor even supported me financially and paid for the MRI scan.
I have been told he may need to be discharged soon, and for us to come back for regular clinic, but I wish my baby and I could remain in the hospital because we live very far, and it might not be possible to attend the scheduled clinics.
Learning points
This is a rare case of large multiple cutaneous melanocytic patches and large melanocytic patches on the scalp.
Early diagnosis and treatment, with surgical excision, are important to reduce chances of malignancy.
Long-term follow-up in a multidisciplinary approach is essential to avoid risk of malignant transformation, reduce disability and improve quality of life.
Ethics statements
Patient consent for publication
Acknowledgments
We thank our colleagues at the neonatal unit, the nurses who took care of the baby and the mother for allowing us to publish this case.
Footnotes
Contributors HM identified the case, wrote the first draft, managed the child clinically, and read and approved the final manuscript. NM reviewed literature and provided inputs in the references and final write-up. MM supervised the case report writing, and read, reviewed and approved the final manuscript. KPM initiated, supervised and reviewed the manuscript, and submitted it on behalf of all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.