Article Text

Abstract
A man in his 30s with alpha thalassaemia (four-alpha globin gene deletion) presented with 1 week of shortness of breath and 1 month of general malaise. Pulse oximetry monitoring revealed low peripheral oxygen saturation of approximately 80% despite maximal high-flow nasal cannula oxygen (fractional inspired oxygen 1.0–60 L/min flow). Arterial blood gas samples were chocolate brown in colour, with a low arterial partial pressure of oxygen of 197 mm Hg. This large oxygen saturation gap raised suspicion for methaemoglobinaemia. However, the patient’s co-oximetry results were suppressed by the blood gas analyser and delayed a definitive diagnosis. A methaemalbumin screen was sent instead, which was positive at 65 mg/L (reference interval: <3 mg/L). Treatment with methylene blue was initiated but did not result in complete resolution of cyanosis. This patient had been red cell exchange dependent since childhood for thalassaemia. Therefore, an urgent red cell exchange was initiated overnight, leading to an improvement in symptoms and interpretability of co-oximetry results. This resulted in rapid improvement without residual sequelae or complications. We conclude that a methaemalbumin screen can be used as a surrogate test for prompt confirmation of diagnosis in lieu of co-oximetry in cases of severe methaemoglobinaemia or in cases with underlying haemoglobinopathy. Red cell exchange can allow prompt methaemoglobinaemia reversal, especially if methylene blue is only partially effective.
- Respiratory system
- Poisoning
- Haematology (incl blood transfusion)
- Adult intensive care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Methaemoglobinaemia is rare and often difficult to diagnose, because routine analytical methods are impaired by the chocolate brown colour of the blood. Patients with inherited haemoglobinopathies, such as alpha thalassaemia, may be prone to developing concomitant haemolysis when exposed to oxidative stress (although rare). In this rare case, this oxidative stress also led to toxic methaemoglobinaemia, resulting in profound cyanosis. A methaemalbumin level may be used as a surrogate confirmation test to avoid delays in treatment of methaemoglobinaemia with methylene blue. Red cell exchange can also be considered to facilitate recovery and return of haemoglobin oxygen-carrying capacity.
Pulse oximetry is a standard oxygen saturation monitoring technique used to estimate arterial blood oxygen saturation (SpO2) based on the light absorbance of oxyhaemoglobin and deoxyhaemoglobin. When low peripheral SpO2 is identified, an arterial blood gas may be used to more accurately assess the partial pressure of oxygen in blood (PaO2). While arterial blood gas sampling usually confirms a similarly low PaO2, in rare cases, the SpO2 and PaO2 are discordant. A normal or elevated PaO2 in the setting of low SpO2 should raise suspicion for a dyshaemoglobinaemia: methaemoglobinaemia, sulfhaemoglobinaemia or cyanide toxicity.1
Methaemoglobinaemia is characterised by elevated methaemoglobin (more than 1%–2% of the total haemoglobin) in blood. In methaemoglobin, the iron in one or more of the four heme groups (normally, ferrous iron, Fe2+) is oxidised to the ferric form (Fe3+), rendering haemoglobin unable to carry oxygen. Methaemoglobin values of 10%–20% cause clinical cyanosis and brown blood but are otherwise well tolerated by the patient. Values over 30% may cause dyspnoea, nausea and tachycardia. Coma may occur when values approach 55%, and values over 70% are thought to be incompatible with life.2 Methaemoglobin in the blood activates an enzymatic reduction process within red blood cells to maintain homeostasis with over 50% ferrous haemoglobin. Clinically, significant levels of methaemoglobin occur when there is a dysfunction with this reductive process or in the presence of oxidants which produce methaemoglobin faster than the body can reduce it.2
Methaemoglobinaemia may be inherited, with symptoms present from a young age, or may be acquired through exposure to oxidising agents or medications. Some of these agents directly oxidise haemoglobin to methaemoglobin while others produce free oxygen radicals, which in turn produce methaemoglobin from haemoglobin. The list of potential agents is lengthy but the most common are local anaesthetics, antimalarial agents, sulfonamide antibiotics or exposure to high levels of nitric oxide, often from ingestion of nitrate-contaminated water.3
The treatment of toxic methaemoglobinaemia consists of methylene blue administration intravenously.4 Methylene blue reduces methaemoglobin to haemoglobin by accelerating the cell’s normal reduction mechanism. If symptoms persist following administration, a subsequent dose can be given after 1 hour. If symptoms persist following two doses, red cell exchange or transfusion may be considered.
Case presentation
A man in his 30s presented with a 1-week history of worsening shortness of breath and 1 month of general malaise, fatigue and weakness. His medical history was notable for alpha thalassaemia major requiring packed red blood cell transfusion every 6–8 weeks, chelation therapy for iron overload, recurrent venous thromboembolism (on apixaban) and hearing impairment. On examination, he had hypoxia with SpO2 of 80%–85%. He was urgently placed on oxygen through a high-flow nasal cannula at fractional inspired oxygen 1.0 and 60 L/min. SpO2 did not increase with this initial therapy. He had mild sinus tachycardia, but was normotensive and afebrile. Further examination showed cyanosis, diaphoresis, and warm and well-perfused extremities. The patient denied any inciting factors, sick contacts, or changes to diet or medications.
Investigations
An arterial blood gas sample was drawn and noted to be chocolate brown in colour. The arterial blood gas showed: pH 7.50, partial pressure of carbon dioxide (PaCO2) 24 mm Hg, PaO2 192 mm Hg, bicarbonate (HCO3) 18 mmol/L, lactate 1.4 mmol/L and SaO2 100%. Co-oximetry results (including methaemoglobin) were unavailable, as the blood gas analyser suppressed them with accompanying spectrum mismatch and turbidity errors.
Blood samples were also sent to the laboratory for testing and revealed haemoglobin 74 g/L, white cell count 7.6×109/L, platelets 316×109/L, sodium 138 mmol/L, potassium 3.4 mmol/L, chloride 108 mmol/L and creatinine 74 µmol/L. A haemolysis screen showed haptoglobin 0.7 g/L (normal), lactate dehydrogenase 808 U/L and bilirubin 53 µmol/L.
Although methaemalbumin testing is not routinely available, we were able to access it through our institution’s on-site laboratory. The patient’s methaemalbumin at presentation was 65 mg/L (reference interval: <3 mg/L), further supporting our presumptive diagnosis of methaemoglobinaemia.
Treatment
The differential diagnosis for the patient’s presentation of hypoxia and cyanosis included methaemoglobinaemia, cyanide poisoning, carbon monoxide poisoning, sulfhaemoglobinaemia, pulmonary embolism and acute heart failure.2 Available clinical and diagnostic evidence was consistent with methaemoglobinaemia. Urgent treatment for presumptive methaemoglobinaemia with methylene blue intravenous infusion (1 mg/kg) was initiated and a second dose was required shortly thereafter. As advised by the poison control centre, concomitant hydroxocobalamin (Cyanokit) was administered intravenously at 70 mg/kg. There were transient decreases in the patient’s SpO2 during methylene blue administration, but his cyanosis and arterial blood gases improved incrementally.
The haematology service was consulted and suggested urgent red cell exchange. The patient was 7 weeks from his last red blood cell transfusion. It was felt that he had a low fraction of remaining haemoglobin A, and that most of this haemoglobin was functionally impaired from methaemoglobinaemia. A red cell exchange was arranged using eight units of antigen negative blood, in keeping with the patient’s usual transfusion regimen.
Outcome and follow-up
After the exchange, arterial blood gas co-oximetry results immediately became available and revealed a methaemoglobin fraction of 0%. The patient’s clinical status rapidly improved, and he was weaned off supplemental oxygen and transferred to the haematology ward the following day. Throughout the patient’s hospitalisation, thorough interrogation of the presenting history was conducted, with no source identified for a cause of methaemoglobinaemia.
Discussion
To our knowledge, this is the first published case of methaemoglobinaemia occurring in a patient with alpha thalassaemia major secondary to haemolysis. Thalassaemia is an inherited condition that results in impaired production of the globin chains within haemoglobin.5 In alpha thalassaemia, mutations in the HBA1 and HBA2 genes cause reduced production of alpha globin chains and, in adults, accumulation of excess beta-like chains. This causes the formation of unstable beta chain tetramers (haemoglobin H) that are susceptible to oxidative injury and leads to increased red blood cell destruction, with the clinical phenotype dependent on the number of affected genes. Alpha thalassaemia major results when all four alpha chain genes are affected. This was once incompatible with life, with most fetuses with this condition born stillborn with hydrops fetalis. However, advances over the last several decades have led to improved treatment.6 Intrauterine transfusions throughout pregnancy can lead to viable pregnancies. In the neonatal period, infants may receive either a bone marrow transplant or be supported with chronic transfusions. Our patient received intrauterine transfusions from early in gestation to delivery, and has been maintained on transfusion exchanges throughout his life.
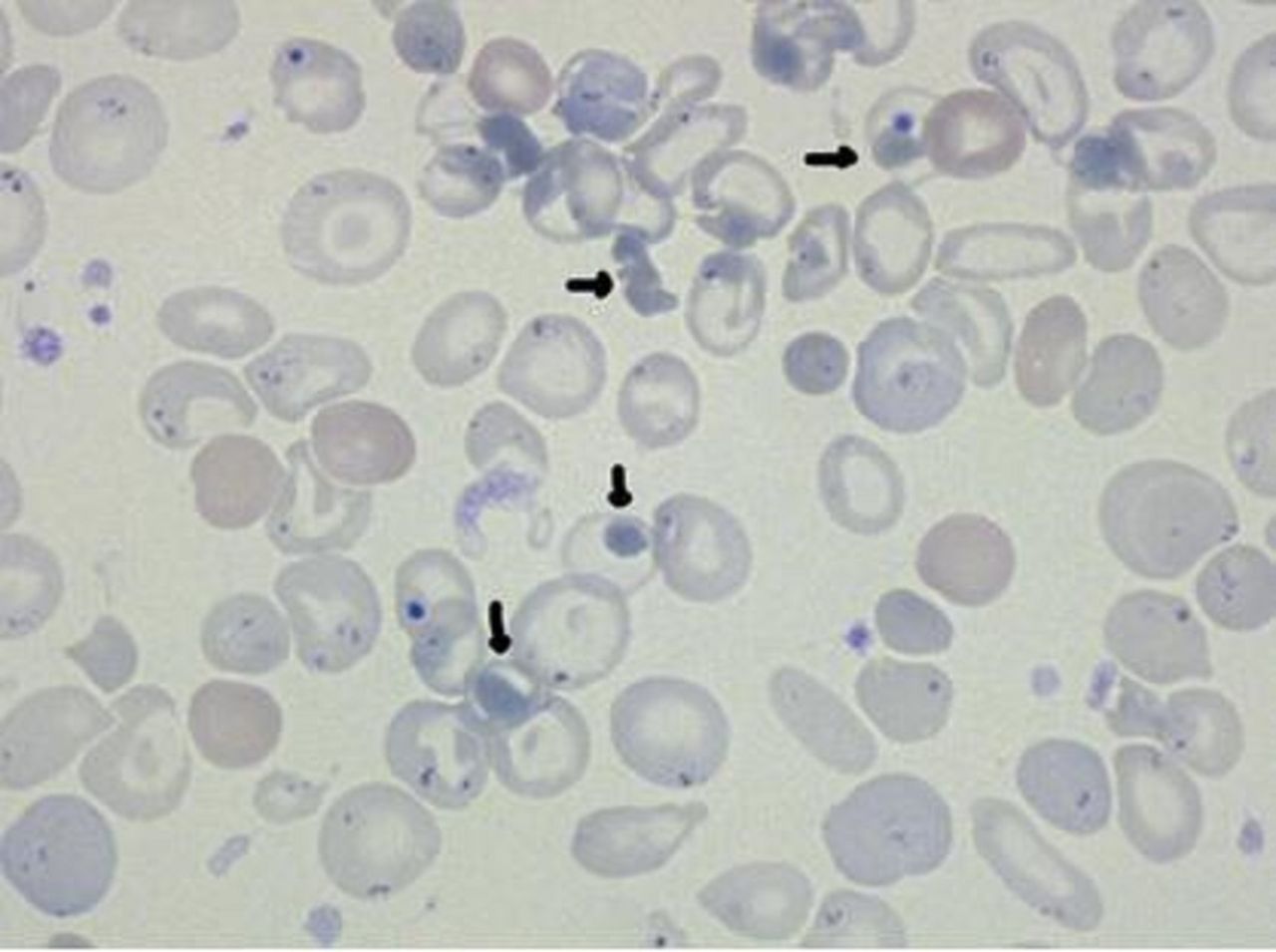
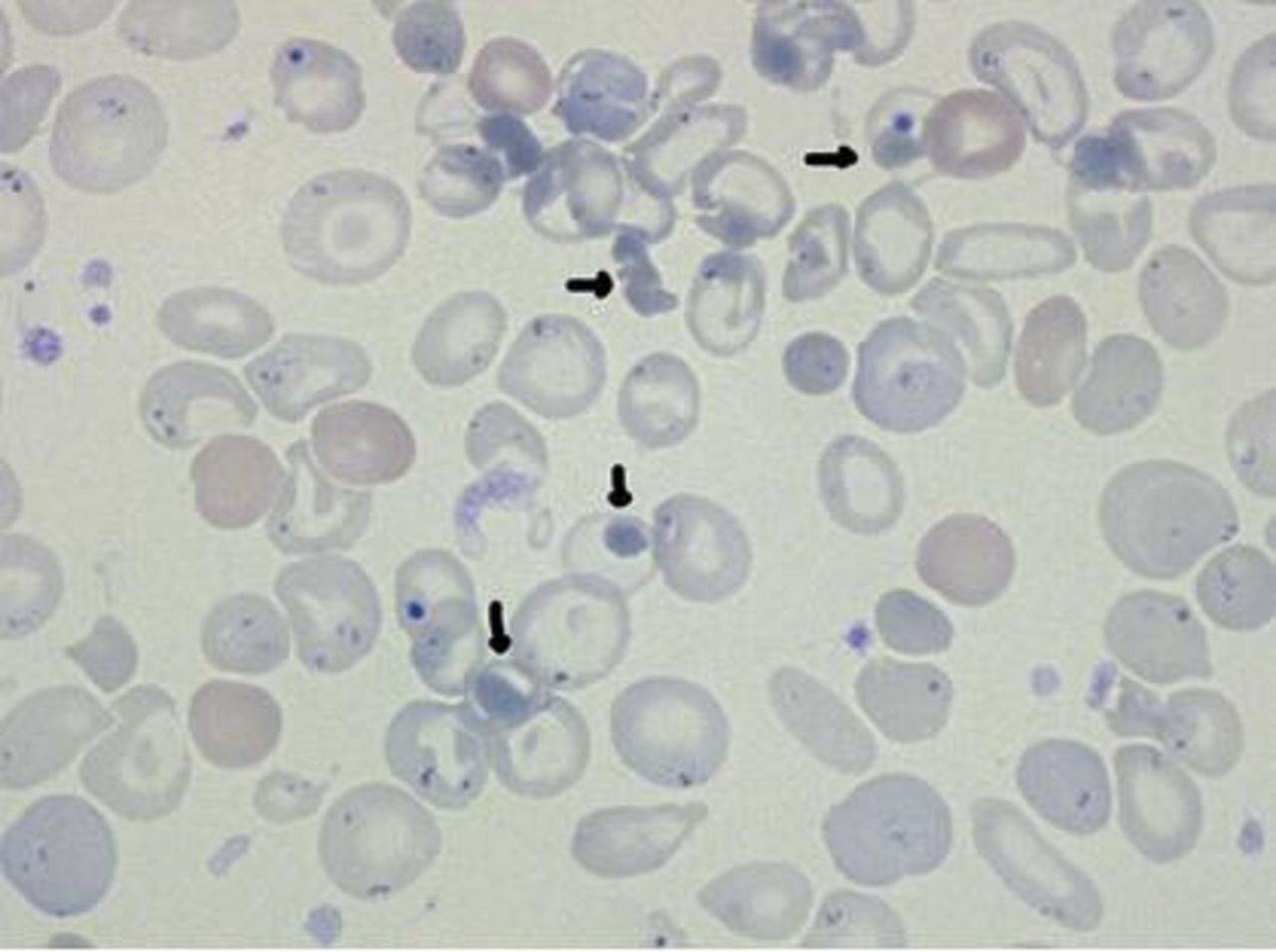
Our patient’s blood film (figure 1) was morphologically consistent with thalassaemia, asplenia (Howell-Jolly bodies) and markedly increased red cell turnover. Large, strikingly dense haemoglobin precipitates were also apparent. Typically, precipitated haemoglobin from haemolysis is present only in limited proportions and requires a special stain (eg, Cresyl blue) to identify small inclusions of denatured haemoglobin (Heinz bodies) throughout the cell.7 However, due to his alpha thalassaemia major, the majority of the patient’s innate haemoglobin consisted of beta chain tetramers. This, in combination with the unidentified oxidative stress causing methaemoglobinaemia, resulted in significant precipitation of haemoglobin observed on the blood film.
{kind=link}
Peripheral blood smear. Large, dense, dark globules marked by black arrow: precipitated haemoglobin.
There is little published on the interaction between thalassaemia and methaemoglobinaemia.8 9 It is hypothesised that patients with abnormal haemoglobin may be at increased risk of developing clinically significant methaemoglobinaemia due to an increased susceptibility to oxidative stress and higher baseline methaemoglobin levels, especially in patients with prior splenectomy or functional asplenia.9 Even in patients without haemoglobinopathies, simple transfusion or red cell exchange has been reported to be beneficial in severe methaemoglobinaemia or when patients not respond to methylene blue.10–14 Interestingly, in our patient’s case, red cell exchange was beneficial for two reasons: (1) it replaced the patient’s abnormal haemoglobin from his alpha thalassaemia major, and (2) it replaced his severe symptomatic methaemoglobinaemia with haemoglobin with normal oxygen-carrying capacity.
Modern benchtop blood gas analysers use a 128-wavelength or 256-wavelength spectrophotometer to determine the total haemoglobin concentration of a blood sample together with the fractional oxyhaemoglobin, deoxyhaemoglobin, carboxyhaemoglobin and methaemoglobin content. The wide availability of these analysers has enabled clinicians to confidently and rapidly diagnose and treat emergent conditions including, but not limited to, methaemoglobinaemia. Similar to other technologies, benchtop blood gas analysers have limitations. The ABL90 FLEX PLUS analysers (Radiometer, Denmark) used by our institution (reportable range: 0%–100%) use an internal algorithm to convert absorbance measurements into a clinically meaningful total haemoglobin concentration and fractional haemoglobin content. The algorithm assumes that the blood sample contains predominantly normal haemoglobin A, although correction for the presence of fetal haemoglobin is possible. Structural haemoglobin variants (eg, haemoglobin M-Boston),15 certain dyshaemoglobins (eg, sulfhaemoglobin)16 and small molecules (eg, hydroxocobalamin,17 methylene blue)18 have all been reported to interfere with the internal algorithm and thereby lead to suppressed co-oximetry results with error flags. The analytical specificity for methaemoglobin is provided in the form of interference testing data but is not reported. The analytical sensitivity is not specified in the manual, although the fractional methaemoglobin is a calculated parameter, and the analyser can report it from 0% to 100%.19
We hypothesise that the primary cause of the suppressed co-oximetry results for our patient was interference by his unusual haemoglobin with the analyser’s internal algorithm. The haemoglobin’s differing absorbance spectrum and its precipitation within red blood cells may both have been contributing factors. Our hypothesis is supported by the observation that co-oximetry results became immediately available after red cell exchange transfusion, which would have replaced any of the patient’s unusual haemoglobin with ‘normal’ haemoglobin A. We cannot rule out that methylene blue and/or hydroxocobalamin also made contributions to the interference, as they were both listed as potential interferences in the ABL90 operator’s manual.19 However, these agents were not yet in the patient’s system when we first encountered the suppressed co-oximetry results.
Although methaemoglobinaemia may be managed effectively without co-oximetry results as demonstrated by our case, a higher degree of confidence in the diagnosis may be obtained through testing for methaemalbumin. This is complex between albumin and oxidised heme, and it forms when the ability of haptoglobin and haemopexin to bind free plasma haemoglobin is exceeded during extensive haemolysis. Methaemoglobin is necessary for methaemalbumin formation, so detectable levels of methaemalbumin in plasma indirectly confirm methaemoglobinaemia.
Learning points
Patients with haemoglobinopathies such as alpha thalassaemia may be prone to developing concomitant haemolysis when exposed to oxidative stress. In this rare case, this oxidative stress also led to methaemoglobinaemia, which resulted in profound cyanosis for this patient.
Haemoglobinopathies may interfere with a spectrophotometer and suppress co-oximetry results needed for diagnosis of methaemoglobinaemia.
To avoid delays in methaemoglobinaemia diagnosis, a methaemalbumin screen may be used as a surrogate test for prompt confirmation of diagnosis in lieu of co-oximetry.
Methylene blue infusion should be initiated to reverse the cyanosis and oxidation of haemoglobin.
Red cell exchange may be required if cyanosis persists after methylene blue administration.
Ethics statements
Patient consent for publication
Acknowledgments
We thank the patient for providing consent to publish his case. We also thank the healthcare team who provided care for him. We also thank Jennifer Croden, Shaun Cowan, Thomas Roston and Lauren Bolster for their help and expertise in drafting this manuscript.
Footnotes
Contributors ZP-C, AIF, TN and VIL all have: (1) made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data; (2) drafted the submitted article and revised it critically for important intellectual content; and (3) provided final approval of the version to be published. Conception, background, data collection and analysis, drafting of the manuscript and revising the manuscript were all done by ZP-C, AIF, TN and VIL.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.