Article Text

Abstract
A woman in her 60s with suspected multicentric Castleman’s disease, who was receiving treatment with oral prednisolone, presented to our hospital with mild cough and malaise. Chest CT showed diffuse infiltrative and granular shadows, indicating exacerbation of lung lesions caused by steroid-resistant multicentric Castleman’s disease. A video-assisted thoracoscopic lung and mediastinal lymph node biopsy was performed. The biopsy revealed mediastinal lymph node tissue consistent with multicentric Castleman’s disease, as well as presence of Cryptococcus neoformans in the alveolar space. C. neoformans infection in immunocompromised individuals may present with diffuse lung lesions and should be noted as a mimicker of acute exacerbation of Castleman’s disease.
- Cryptococcus
- Pneumonia (infectious disease)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Castleman’s disease is a benign lymphoproliferative disorder characterised by hyperplastic lymph nodes.1 The pathogenesis of multicentric Castleman’s disease is attributed to overproduction of interleukin-6 (IL-6) by germinal centre B cells. Furthermore, multicentric Castleman’s disease is occasionally associated with elevated levels of serum IgG4, complicating its distinguishment from IgG4-related disease.2 Infection with HIV is also closely associated with the development of human herpesvirus-8-related diseases, such as Kaposi’s sarcoma; Kaposi’s sarcoma-associated inflammatory syndrome was recently described as a human herpesvirus-8-related disease.3 4 Kaposi’s sarcoma-associated inflammatory syndrome presents with varying degrees of lymphadenopathy, pancytopenia and signs of systemic inflammatory syndrome, rendering it clinically indistinguishable from multicentric Castleman’s disease. Numerous studies have shown that multicentric Castleman’s disease is frequently resistant to treatment with corticosteroids.5 Nonetheless, treatment with steroids is effective against IgG4-related disease. Multiple differential diagnoses should be considered for patients with suspected multicentric Castleman’s disease receiving long-term treatment with steroids who develop respiratory symptoms with bilateral diffuse lung consolidation and granular shadows. These symptoms indicate steroid-resistant multicentric Castleman’s disease, worsening the differential diagnosis of multicentric Castleman’s disease and opportunistic infections. In particular, infection with Cryptococcus presents with a variety of imaging findings in patients with compromised T cell immunity. Furthermore, it is difficult to distinguish exacerbation of steroid-resistant multicentric Castleman’s disease from cryptococcal infections through imaging analysis.
Case presentation
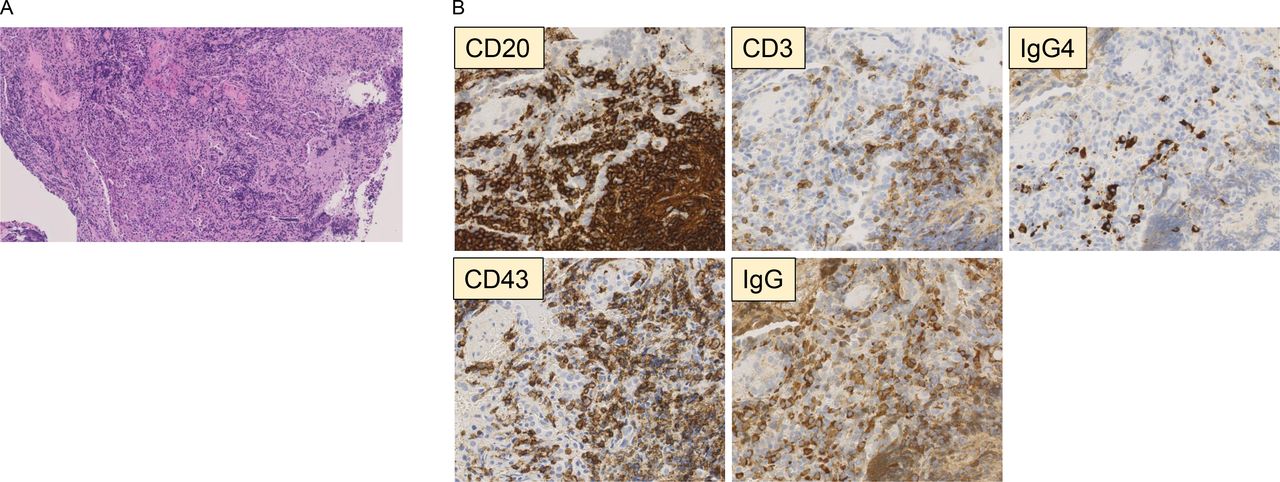
A woman in her 60s with a medical history of type 2 diabetes and hypertension presented with mild cough and general malaise. Seven years earlier, she had visited the Department of Haematology for hyper-γ-globulinaemia and hypercalcaemia with malaise. Eventually, the patient was diagnosed with polyclonal hyper-γ-globulinaemia rather than multiple myeloma. Multiple lung lesions were detected, and the patient was referred to the Department of Respiratory Medicine. CT showed multiple centrilobular granular shadows of the lobules and nodular shadows in both lungs, as well as swelling of the mediastinal lymph nodes (figure 1). In addition, she had elevated levels of IgG4 and IL-6. Four years earlier, 18F-fluorodeoxyglucose (FDG) positron emission tomography-CT showed mild FDG accumulation in the lung nodules, as well as in the mediastinal and hilar lymph nodes. Moreover, strong FDG accumulation was detected in the palatine tonsils. However, biopsy tissue of the palatine tonsils did not reveal notable abnormalities. Three years earlier, a transbronchial lung biopsy was performed. Dense inflammatory cell infiltration was observed in areas thought to be bronchial vascular bundles and alveolar septa (figure 2). The infiltrating cells were mostly lymphocytes, along with a limited number of plasma cells. Individual cells did not show signs of dysplasia, and there was no evidence of a lymphoepithelial lesion. Immunostaining revealed a mixture of B and T cells, with predominance of the former type. There was no light chain restriction, and chain-positive cells were mixed. There were more CD43-positive cells than CD3-positive cells, and there was positivity for cells other than lymphocytes; hence, it was not possible to determine the malignancy. The IgG4/IgG-positive cell ratio was 10%–20%. Clonal cell proliferation was not demonstrated, and the low IgG4/IgG-positive cell ratio was not suggestive of malignant lymphoma or IgG4-related disease. Based on the above results, multicentric Castleman’s disease was strongly suspected. Six months earlier, treatment with oral prednisolone (30 mg/day) had been initiated owing to mild anaemia and cough. A CT scan at the time of the present visit revealed diffuse infiltrative, nodular and granular shadows in both lungs (figure 3).

CT of the chest lung window. Multiple centrilobular granular shadows and nodular shadows in both lungs and swelling of the mediastinal lymph nodes were observed.
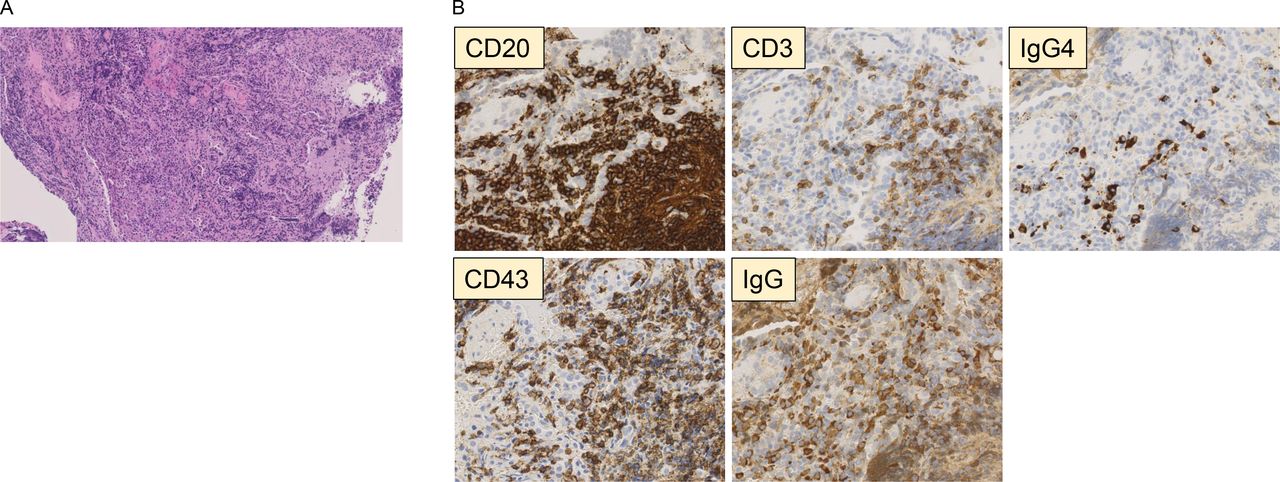
Histopathological findings in tissue obtained from the right lung. (A) Extensive proliferation of lymphocytes in areas of bronchial vascular bundles and alveolar septa (H&E staining) was recorded. (B) Immunohistochemical analysis showed a mixture of B and T cells. There were more CD43-positive cells than CD3-positive cells. The IgG4/IgG ratio was 10%–20%.

CT of the chest lung window. Exacerbation of multiple lung lesions 6 months after steroid therapy was noted.
Investigations
Laboratory tests yielded the following results: leucocyte count, 11 .01×109/L (with neutrophils accounting for 84% of the total number); C reactive protein (CRP), 5 mg/dL (reference range: <1.0 mg/dL); erythrocyte sedimentation rate, 116/hour (indicating inflammation); haemoglobin, 108 g/L; serum protein, 11.5 g/dL; and albumin, 2.5 g/dL. In addition, there was an increase in polyclonal γ-globulin in the protein fraction (ie, IgG: 5952 mg/dL; IgM: 213 mg/dL; IgA: 881 mg/dL and IgG4: 710 mg/dL). The level of haemoglobin A1c was 7.1%. The level of IL-6 increased to 15.6 pg/mL (reference range: <7 pg/dL). The free light chain was not skewed. The results of the HIV-1/2 antigen and antibody screening test were negative.
A month after this visit, a video-assisted thoracoscopic surgery biopsy of the lungs and mediastinal lymph nodes was performed to confirm the diagnosis. Grocott’s staining revealed numerous black yeast-like fungi and giant cells in the airspace (figure 4). Polynuclear giant cells contained fungi that stained red with Periodic acid–Schiff stain and blue with Alcian blue stain. A growing fungus was found in the vacuole of giant cells, where it produced mucous substances. There were no epithelioid cell granulomas, suggesting that steroid therapy was ineffective in inducing cell-mediated immunity against yeast. A panfungal PCR test was performed using paraffin sections, and 100% homology with C. neoformans was obtained; thus, the lung lesion was recognised as pneumonia caused by C. neoformans.
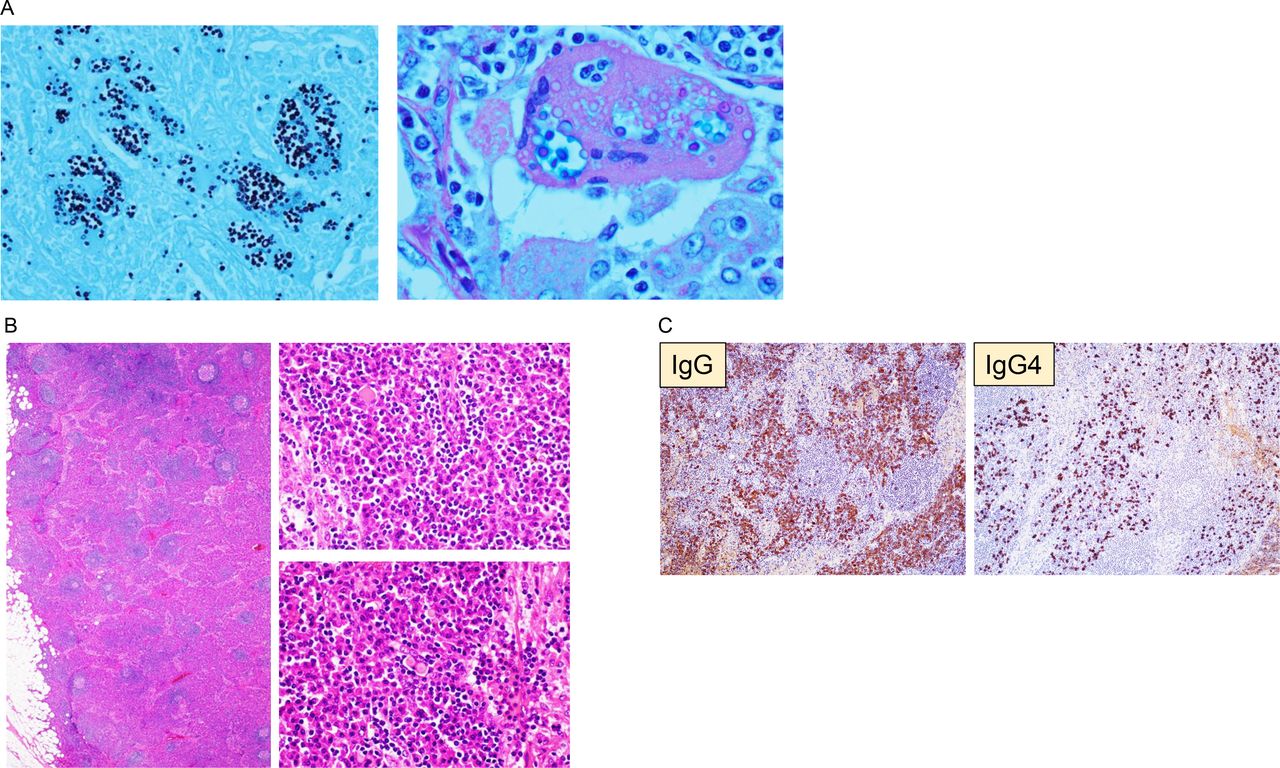
Histopathological findings in tissue obtained from the right lung tissue and the mediastinal lymph nodes. (A) Presence of numerous black yeast-like fungi and giant cells in the airspace (Grocott’s staining: lung tissue) was observed. (B) Presence of numerous lymphoid follicles with germinal centres (H&E staining: mediastinal lymph node) was noted. (C) The IgG/IgG4 ratio was approximately 40%–50% (immunostaining: lymph node).
In the mediastinal lymph node tissue (short-axis diameter: >1.5 cm), numerous lymphoid follicles with germinal centres were found. The spaces between the follicles were slightly reddish and enlarged. Most of the inflammatory cells were plasma cells, and numerous Russell bodies were found. A large amount of immunoglobulins was produced. In immunostaining, the IgG/IgG4 ratio was approximately 40%–50%. Both IgG4 and IL-6 levels were elevated; therefore, it was necessary to distinguish between multicentric Castleman’s disease and IgG4-related disease. The serum CRP levels were increased to 5.45 mg/dL (reference value: 0.80 mg/dL); the levels of IgA were 881 mg/dL (reference value: 330 mg/dL). There was no atopy predisposition observed, and lesions were distributed in both lungs and mediastinal lymph nodes. However, they were not found in the eyes, lacrimal glands/salivary glands or pancreas. PCR testing using whole blood did not detect human herpesvirus-8 DNA. There was positivity for cryptococcal antigen in the serum, but not in the cerebrospinal fluid; moreover, the cerebrospinal fluid culture was negative. Consequently, this patient was diagnosed with multicentric Castleman’s disease complicated by cryptococcal pneumonia.
Treatment
Oral treatment with fluconazole (400 mg/day) was initiated as treatment for lung-only infection. Currently, the dose of prednisolone is gradually reduced, and treatment with this agent will eventually be discontinued after 12 months.
Outcome and follow-up
A CT scan performed 4 months after initiating the anti-fungal treatment showed improvement in the lung lesions; however, the lung lesions attributed to multicentric Castleman’s disease persisted (figure 5). We are currently considering to add tocilizumab for the treatment of multicentric Castleman’s disease.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CT of the chest lung window performed 4 months after the initiation of anti-fungal treatment.
Discussion
This case report emphasises two points: (1) the differentiation between IgG4-related disease and multicentric Castleman’s disease; and (2) the differentiation between cryptococcal pneumonia and diffuse lung disease in immunocompromised individuals.
Multicentric Castleman’s disease involves the overproduction of IL-6 by the lymph nodes. IL-6 differentiates B cells into plasma cells to produce immunoglobulins, resulting in elevated serum IgG4 levels and IgG4-positive plasma cell infiltration. The histological findings of IgG4-related disease are similar to those of Castleman’s disease (type I).6 Hence, it is necessary to differentiate IgG4-related disease with lymph node lesions from the plasma cell type of Castleman’s disease. For the reasons stated above, it is difficult to distinguish between multicentric Castleman’s disease and IgG4-related disease using the IgG4/IgG ratio.7
Clinical studies have examined markers that could be useful for the differentiation of these diseases. Despite increases in IgG and IgE, CRP or globulins are not increased in IgG4-related disease. According to the results of a study,8 the presence of the following findings are indicative of multicentric Castleman’s disease: serum CRP >0.8 mg/dL; IgA >330 mg/dL, absence of atopy predisposition, and no involvement of the eye, lacrimal gland/salivary gland, or pancreas in the lesion.
In immunocompromised patients, cryptococcal pneumonia can cause diffuse lung disease. Furthermore, in the absence of response to steroid therapy, it is important to distinguish C. neoformans infection from exacerbation of multicentric Castleman’s disease. In a study of 151 patients without HIV with pulmonary cryptococcosis in Japan, 84 patients had underlying disease; diabetes was found in 32.1% of the patients; moreover, steroid users accounted for 37% of the population.9 Steroids suppress T cells, particularly CD4+ T helper cells.10 T helper 1 cells control immunity against intracellular parasites by producing interferon-γ, and steroids exert a marked effect on these cells. Thus far, there are few reports of multicentric Castleman’s disease associated with cryptococcal infection. A search conducted using the MEDLINE database yielded only disseminated cases that occurred during treatment with tocilizumab and cases of cryptococcal tendonitis.11
C. neoformans lung lesions are generally more extensive in immunocompromised individuals versus immunocompetent individuals.12 13 These are characterised by multiple nodules located immediately below the peripheral lung and pleura, infiltrative shadows, cavity shadows, bilateral pneumonia and occasionally diffuse granular shadows; in addition, histological analysis may not reveal a granulomatous reaction.
C. neoformans lung disease is classified into four patterns based on the formation of granuloma and the degree of inflammation.14 Granulomatous inflammation controls the growth of C. neoformans in static lesions. However, there is no inflammatory response in patients with severe cellular immunodeficiency (eg, HIV), and a large amount of C. neoformans is present in the alveoli, interstitium and capillaries. In the present case, cellular immunodeficiency was noted following the administration of steroid therapy, diabetes was present and there was no observation of granuloma formation. Granulomatous pneumonia with immunodeficiency owing to inflammatory cell infiltration and polynuclear mobility was considered.
Learning points
The serum levels of IgG4 are elevated in some cases of multicentric Castleman’s disease; differentiation from IgG4-related disease using case clinical data is necessary.
Cryptococcosis in immunocompromised individuals presents with a variety of imaging findings.
Differential diagnosis (eg, Cryptococcus neoformans pneumonia) for diffuse parenchymal lung disease, such as multicentric Castleman’s disease, should be considered.
Ethics statements
Patient consent for publication
Footnotes
Contributors JT, HT, KK and YK (1) made substantial contributions to the study concept or the data analysis or interpretation; (2) drafted the manuscript or revised it critically for important intellectual content; (3) approved the final version of the manuscript to be published and (4) agreed to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.