Article Text

Abstract
By definition, anteroposterior (AP) compression type 1 (APC-1) injury is a type of pelvic ring injury, which is widely acknowledged as ‘stable’. Unstable forms of this injury are very rare and present a challenge for diagnosis and clinical management. Detailed herein is a man in his early 30s, referred to our institution with a 2-year history of pubic symphysis pain following a road traffic accident. Radiological investigation revealed an unstable APC-1 injury. This was subsequently managed with surgical reconstruction leading to the successful return of the patient to former function and recreational activities.
- Orthopaedic and trauma surgery
- Orthopaedics
- Trauma
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Fractures and injuries of the pelvic ring account for 2%–8% of all fractures and are usually caused by high-energy trauma incidents, such as car accidents and falls from a height.1–3 They are much more common in polytraumatised patients (incidence approximately 30/100 000 per capita).3 4
The Young and Burgess classification for pelvic fractures is one of the most widely used by trauma surgeons5 as it considers injury mechanism (type, severity and direction of force), the degree of joint instability and treatment modality.6 7 This system describes four broad categories of injury mechanism: anteroposterior (AP) compression (APC), lateral compression, vertical shear and one which has combined features of the other three. This case concerns the APC category which is divided into three subgroups: APC-1 describes a stable injury in which the pubic symphysis diastasis (PSD) is <2.5 cm and both anterior sacroiliac (SI) joint and pelvic floor ligaments are intact; APC-2 is only partially stable with SI disruption and a PSD of >2.5 cm and APC-3 injuries are completely unstable in which there is SI ligament shearing in addition to a PSD of >2.5 cm.8
We present a male patient who was previously diagnosed with a traumatic APC-1 injury and who continued to have pelvic pain and weakness 2 years later. To the best of our knowledge, this is the only reported case of an unstable APC-1 injury (as defined by a PSD of <2.5 cm). In addition, having failed to improve with non-operative management, he was successfully treated surgically to regain full, pain-free mobility.
Case presentation
A previously fit-and-well office worker in his early 30s presented to our institution for the evaluation of pubic symphysis pain. His symptoms began after a road traffic accident 2 years previously following which he was seen and examined at the local district general hospital. On examination, he complained of pubic symphysis discomfort, and radiographs of his pelvis revealed an APC-1 fracture type (figure 1). He was reassured and discharged home with advice to mobilise with a Zimmer frame and to attend physiotherapy treatment sessions in line with the guidelines by Young and Burgess.8 Despite this, his symptoms did not improve resulting in a decline in his mental state.

Anteroposterior pelvic radiograph at original presentation, demonstrating a pubic symphysis diastasis of <2.5 cm (white arrow) and no left sacroiliac joint widening (red arrow).
Prior to his accident, the patient had been very active, participating in gym-based weight training and running four times a week. However, over the last 2 years, pain and weakness in his pelvic girdle had reduced his ability to participate in these activities.
On presentation to our centre, his case was re-evaluated. Of note, the physical examination highlighted the presence of pain in the pubis and left SI joint. A positive flexion, abduction and external rotation (FABER) test result was elicited (pain on provocation testing) on the same side, with normal hip movement. No leg length discrepancy was found, and neurovascular function was symmetrical and intact throughout both lower limbs.
Investigations
New AP pelvic X-rays were obtained, in addition to ‘flamingo’ views (dynamic stress imaging) (figure 2). In these more recent images, a calcification at the upper margin of the pubic symphysis was demonstrated, in addition to the right hemipelvis being more proximately located relative to the left by approximately 6 mm in a neutral position. Furthermore, there also appeared to be some loss of alignment at the left SI joint; with the left leg raised on flamingo view, there was an exacerbation of vertical translation of the pubic ramus up to 14 mm, consistent with mechanical instability. Blood results were unremarkable. Based on the previous and current findings, the diagnosis of an unstable APC-1 pelvic ring fracture was established.
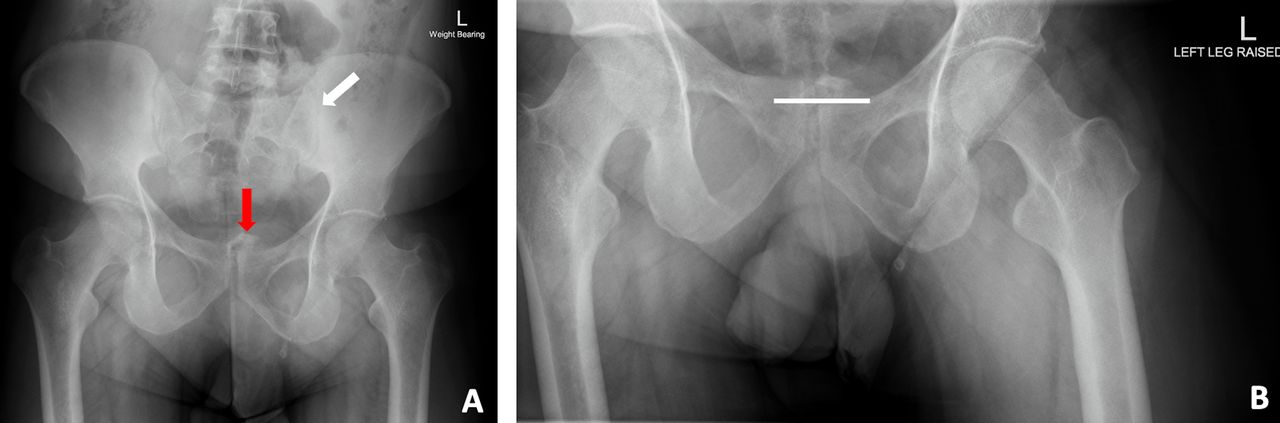
Anteroposterior (A) and flamingo (B) pelvic radiographs on presentation to our centre 2 years post trauma. These views demonstrate: (A) a calcification at the upper margin of the pubic symphysis (red arrow) and instability at the left sacroiliac joint (white arrow) and (B) vertical translation of right hemipelvis (white line).
Treatment
Due to the previous failure of non-operative management, the patient was offered and elected to undergo pubic symphysis fusion, using a bone graft and plate,9 and left posterior pelvic fixation by inserting a SI joint screw. Initially, an examination under anaesthesia (EUA) was performed, to further assess the pelvic ring instability before definitive fixation. This examination involved placing stress on the pelvic ring; with the patient in a supine position and abducting his hips, instability of the pelvis was demonstrated (figure 3).

Stress X-rays obtained on examination under anaesthesia in theatre, further highlighting a pubic symphysis diastasis of 1.5 cm (white arrow) and instability at the left sacroiliac joint (red arrow).
A standard Pfannenstiel incision was made, to expose the rectus muscle medially. This muscle was then longitudinally incised, elevated from its insertion point and laterally retracted to allow for visualisation of the pubic symphysis. The bladder was exposed and protected throughout the surgical procedure. Tricortical iliac bone graft from the left iliac crest was used to pack the pubic symphysis gap, and a 3.5 mm, eight-hole Matta plate was used for compression (figure 4). A left SI joint screw was percutaneously applied. Finally, the iliac crest defect from the harvested site was reconstructed with a bovine xenograft (Tutobone), fixed with two iliac screws (figure 5).

Intraoperative images showing: (A) the removal of the tricortical bone graft from the iliac crest and (B) pubic symphysis fusion using this graft and an eight-hole Matta plate.

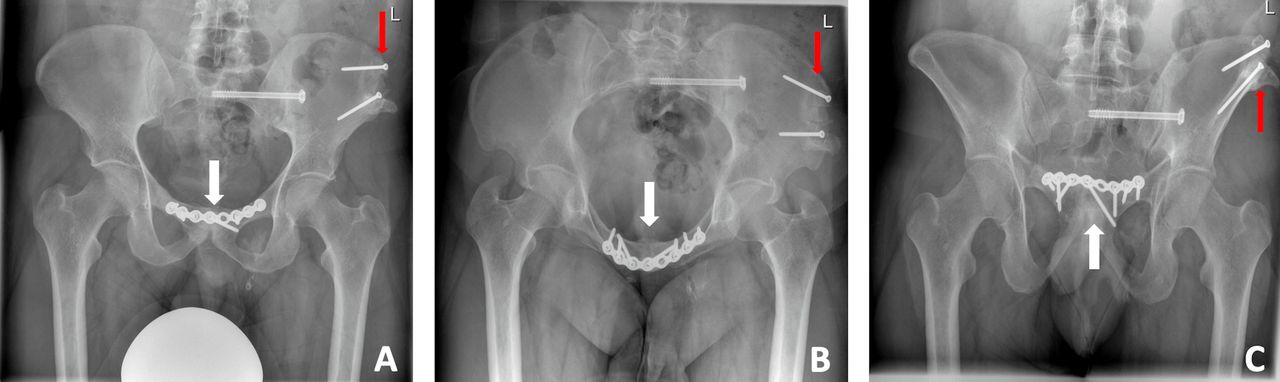
Postoperative anteroposterior (A), inlet (B) and outlet (C) radiograph views of the pelvis, demonstrating pubic symphysis fusion with a bone graft and plate (white arrows) and the insertion of a left sacroiliac joint screw (red arrows).
Immediate, postoperative care involved immobilisation in a wheelchair for 9 weeks and thromboprophylaxis (Tinzaparin 6000 units/day) treatment for a period of 12 weeks. He then progressed to using a Zimmer frame at 8 weeks, then bilateral elbow crutches, before embarking on physical therapy, to improve hip mobility and rebuild and reinforce pelvic floor and lumbar spine muscles. Full pain-free weight bearing was achieved at 5 months; the patient was allowed to resume all types of physical activity, such as swimming, cycling and light weight training.
Outcome and follow-up
At the 14-month follow-up appointment, the patient was pain-free and had regained full mobility. He had resumed participation in all former recreational activities. Final X-ray imaging demonstrated complete consolidation of the pubic fusion and integration of the xenograft at the left iliac crest (figure 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Anteroposterior (A), inlet (B) and outlet (C) pelvic radiograph views obtained at 14-month follow-up, showing successful pubic symphysis fusion (white arrows) and full integration of the xenograft at the left iliac crest (red arrows), as well as an intact left sacroiliac joint screw.
Discussion
Identifying the correct type of pelvic ring injury is fundamental to the management of trauma patients. This case highlights that some patients may occasionally be misrepresented using the Young and Burgess classification, which may have implications for patient management and outcome.
The pelvis is composed of paired innominate bones (ilium, ischium and pubis) and the sacrum. These are arranged in a ring-like structure which serve to transfer weight of the upper skeleton to the lower body and provide attachment to locomotive muscles and ligaments.10 Pelvic ring stability is dependent on the integrity of specific ligaments that connect the three bones together. In normal situations, these ligaments aim to withstand physiological stresses and maintain the fundamental pelvic structure; however, these structures can be vulnerable to trauma.
There are several ligaments relevant to pelvic ring injury, each having their own specific function. Anteriorly, the superior and inferior pubic ligaments are largely responsible for holding the pubic symphysis together; these ligaments help maintain a normal PSD of <2.5 cm.8 11 More laterally, the sacrotuberous and sacrospinous ligaments create a portion of the pelvic floor both of which connect the sacrum to the ischium to provide rotational stability and opposition to vertical shear and flexion forces. Posteriorly, the anterior and posterior SI ligaments provide stability for the SI joints, with the latter being considered the most important in maintaining the sacrum in its normal anatomical position.12
Knowledge of these structures is pivotal in understanding the skeletal consequences of pelvic ring injuries. In our patient, immediately post injury, AP radiographs showed he had a PSD of 7.3 mm which is well within the normal range. There was also no evidence of SI joint widening. These points suggest that there was no ligamentous disruption and support the initial claim that the injury was a ‘stable’ APC-1 injury. This is also in keeping with the benign nature of his symptoms and the fact that he was able to mobilise without difficulty. As a consequence of his original injury classification, the patient was managed non-operatively. However, having completed a prolonged rehabilitation programme, his symptoms clearly did not settle leading him to present to our centre 2 years later.
At this second presentation, flamingo pelvic views13 and views under EUA were performed for the first time. It was observed on EUA that the PSD was wider than previously noted on the original AP view (7.3 mm increased to 1.5 cm), but this was still within the normal range (<2.5 cm) and remained consistent with an APC-1 injury type.8 Doro et al14 have previously questioned the validity of the 2.5 cm gap and postulated that posterolateral ligament disruption may even occur at less than this distance. Incidentally, the same authors suggested that in PSD lesions of <1.5 cm, this ligament damage was unlikely.14 However, despite this, in our case both radiographic investigations revealed pelvic instability at the position of the left SI joint, suggesting a compromise of at least one of the anterior SI joint ligaments.15
The case highlights that standard unstressed single-view pelvic radiographs sometimes may be insufficient to reveal more subtle, but clinically relevant, radiographic abnormalities. The current standard is to perform AP pelvic X-rays as in our patient’s case, and in the context of mild symptoms, there would have been little evidence to recommend specialist views at initial presentation. Interestingly, Gardner et al have reported that pelvic AP radiographs may under-represent pelvic injuries due to compression secondary to pelvic binding or ‘recoil’ which may have occurred.16 In addition, it has previously been noted that in some individuals EUA may be required to demonstrate a PSD widening of over 2.5 cm.17 18 The above factors may explain the reported 6% of incorrectly classified pelvic ring injuries diagnosed using single static AP radiographs.8 However, in our case, the PSD remained <2.5 cm despite stressed and unstressed imaging.
The pubic symphysis is the weakest part of the pelvic ring and tends to be compromised first in injury.19 In our patient, it was surprising to find that he had instability elsewhere in the pelvic ring given a normal PSD distance. We hypothesise therefore that on original injury, the ligaments surrounding the SI joint may have been bruised or fibres partially damaged, causing mild instability which was undetected on standard radiographs. Again, without complete damage to these ligaments, this was consistent with a diagnosis of an APC-1 injury. However, over time, with regular physiotherapy and the continuation of impact sporting activities, there may have been a progressive increase in laxity at the left SI joint and failure of the anterior pubic symphysis ligaments to heal, which could explain why after 2 years, widening of this joint and worsening of symptoms was demonstrated. Consequently, our strategy to proceed with fusion of the pubic symphysis and insertion of the left SI joint screw provided mechanical stability to the pelvic ring and successful resolution of his chronic symptoms, with pain-free mobility at 14-month follow-up.
An additional finding which was not visible on the original AP pelvic radiographs was the presence of ectopic bone formation on the superior margin of the pubic symphysis. This could be attributed to the recurrent stress or compression forces on a chronically unstable joint or repetitive microtrauma, haematoma formation and ossification of the ligaments.20 21 Interestingly, a previous study of APC-2 injuries demonstrated partial ossification of pelvic ligaments, but the prevalence at which this occurs in other APC injury types is unknown.21
In summary, as this patient was diagnosed with an APC-1 injury, the expectation was that his symptoms would have improved with conservative management. In reality, that was not observed and therefore, this case demonstrates that there is a potential subset of APC-1 injuries requiring surgical consideration for symptomatic relief and functional improvement, as seen in this patient. There is currently a paucity of data regarding the long-term outcome of patients managed for APC-1 lesions and therefore we would recommend that further follow-up work is performed in this area.
Patient’s perspective
I have always been very active and practical, going to the gym four times a week and do some mechanic work and DIY on the weekends. When my accident happened, I became increasingly worried about how unstable my pelvis felt, so I stopped doing exercise and the hobbies I loved: this really affected my confidence, and I became very hesitant to socialise. I went from being really independent to relying on people for help, especially as I found it painful to sit down. After my operation, I am 99% back to normal; I feel great and am comfortable in myself. I am pain-free and have returned back to the gym and go running when I can. I am extremely grateful to the team of doctors who were able to help me.
Learning points
Despite anteroposterior compression type 1 (APC-1) pelvic injuries being widely recognised as stable, it is important to acknowledge that unstable APC-1 injuries may also exist.
Unstable APC-1 injuries can cause significant ongoing pain and disability, and in these cases, follow-up with additional imaging should be considered.
Failure of conservative management due to mechanical instability would require surgical intervention in the form of pubic symphysis fusion for restoration of function and symptomatic relief of chronic pain.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors SMW: literature search, collected clinical data and prepared the manuscript. VG: proof-read the manuscript. MM: literature search. PVG: original concept, performed surgery and proof-read the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.