Article Text

Abstract
Adult-onset Still’s disease (AOSD) is a rare systemic autoinflammatory disease with a broad spectrum of clinical manifestations including fever, skin rash, arthralgia and neutrophilic leucocytosis. Small bowel inflammation in AOSD has been reported in association with Crohn’s disease, coeliac disease and chronic intestinal pseudo-obstruction. We have here reported the first-time case of AOSD with small bowel involvement, presenting with chronic vomiting. Fluorodeoxyglucose total-body positron emission tomography/CT showed high uptake of the duodenum and first jejunal loop. Faecal calprotectin increased. Duodenal histology revealed neutrophilic infiltrate among duodenal enterocytes and severe chronic lymphoplasmacellular infiltrate of the lamina propria. Vomiting disappeared when duodenojejunal inflammation was controlled by immunomodulatory treatments for AOSD, suggesting a possible causal relation between duodenojejunal inflammation and the symptom.
- Gastroenterology
- Stomach and duodenum
- Rheumatology
- Endoscopy
- Drugs: gastrointestinal system
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Adult-onset Still’s disease (AOSD) is a rare systemic autoinflammatory disease characterised by intense activation of the innate immune cells (macrophages, neutrophils) and overproduction of proinflammatory cytokines (interleukin (IL)-1, IL-6, IL-18) in response to infections or chemical substances leading to tissue damage. The most common clinical manifestations of AOSD are fever, skin rash, arthritis and arthralgia. Less common manifestations are odynophagia, myositis and myalgia, enlargement of lymph nodes and spleen, myocarditis and pericarditis, pleuritis, hepatitis and coagulation disorders. The most severe cases can evolve to life-threatening conditions, such as fulminant hepatitis, macrophage activation syndrome, respiratory distress syndrome and disseminated intravascular coagulation. Laboratory investigations usually reveal leucocytosis with neutrophilia, raised ferritin, elevated C reactive protein (CRP) and erythrocyte sedimentation rate.1 Small bowel involvement has been reported only in a few cases in association with Crohn’s disease, coeliac disease and chronic intestinal pseudo-obstruction.2–7
Case presentation and investigations
A woman in her 60s presented with chronic vomiting at our gastroenterology outpatient clinic 2 years ago. The symptom had been present for 5 months, not preceded by nausea and occurring in the late post-prandial period, 1–2 hours after meals. Non-bloody diarrhoea (three bowel movements/day, Bristol Index 6) and 7 kg weight loss (from 50 kg down to 43 kg; body mass index 16.5) were also reported.
AOSD had been diagnosed 3 years earlier at the rheumatology department. The patient had been treated first with steroids and methotrexate, then with anakinra and finally with low-dose steroids and canakinumab (a monoclonal antibody against IL-1ß) in the last year. She had also suffered from a breast neoplasm 7 years before presentation, treated with surgery, radiotherapy and tamoxifen, with complete recovery.
At the time of presentation, the patient was on therapy with canakinumab 150 mg once a month, prednisone 10 mg daily and calcium carbonate 1 g for concurrent steroid treatment, ramipril 2.5 mg for mild hypertension, trazodone 50 mg for mild depression and rabeprazole 20 mg.
Since the onset of vomiting, she had undergone several investigations. Laboratory tests showed normal white cell count and haemoglobin, raised transaminases (two times upper normal limit), increased levels of pancreatic enzymes (three times upper normal limit) and increased CRP (three times upper normal limit). Coeliac disease was excluded by the normal values of anti-transglutaminase antibodies; immunoglobulins IgA, IgG and IgM were in their normal range. Thyroid function and glycaemia were normal. Major and minor hepatotropic viruses were absent. Alpha-1-antitrypsin, iron and copper metabolism were normal. Hepatic autoantibodies were absent. Faecal elastase was slightly decreased.
An upper gastrointestinal endoscopy was described as unremarkable, with normal gastric biopsies. The Helicobacter pylori antigen was absent in the faecal sample. Colonoscopy with retrograde ileoscopy including mucosal biopsies was normal. Abdominal CT and abdominal MRI with contrast media showed only biliary sludge and two small pancreatic cysts. Abdominal ultrasound performed with a high-frequency probe noted a thickened concentric duodenal wall (7 mm), but the finding was not confirmed by subsequent endoscopic ultrasound.
The patient was treated with domperidone 10 mg three times a day and then levosulpiride 25 mg two times per day with no clinical improvement.
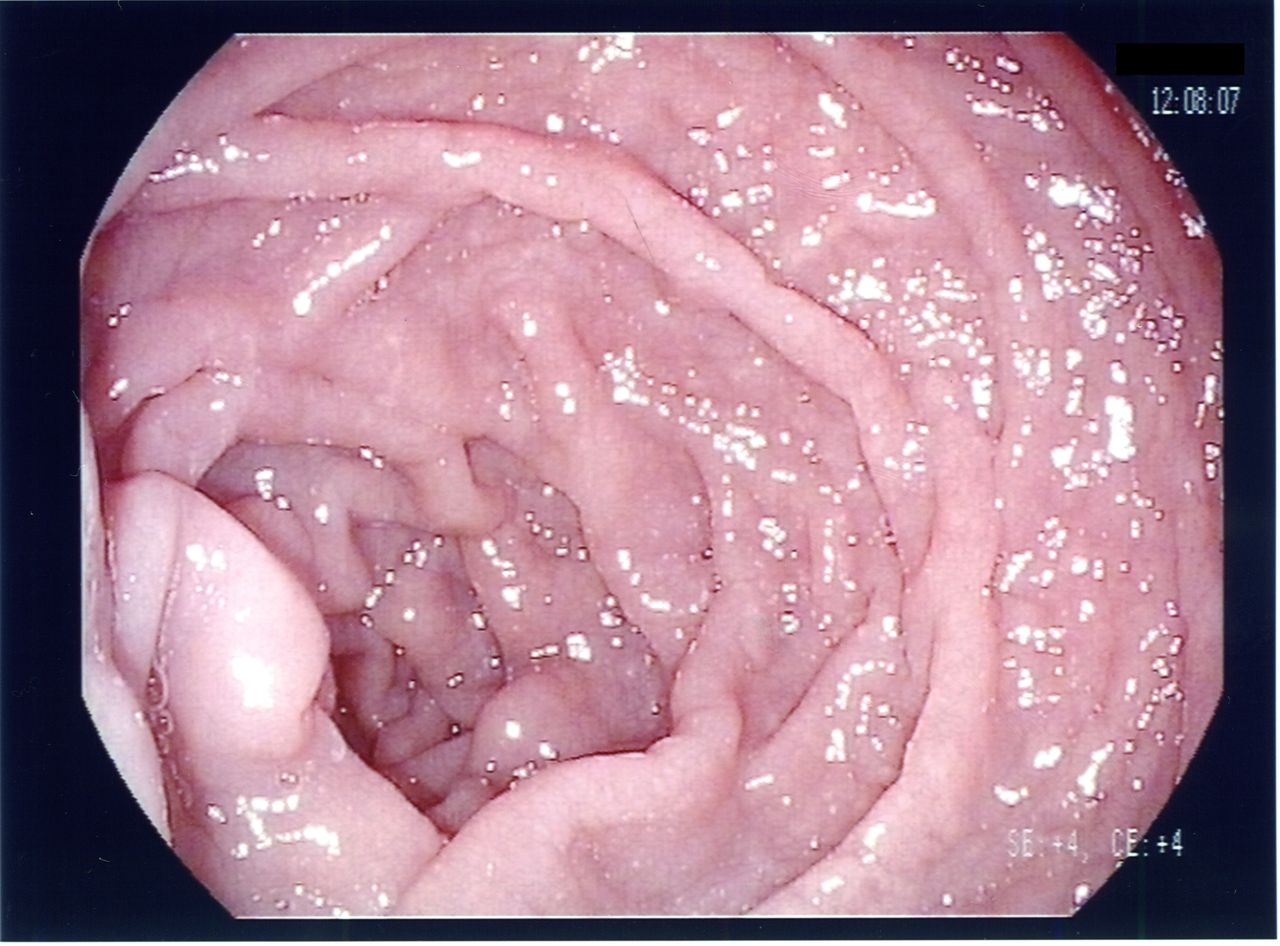
She was hospitalised in our gastrointestinal unit 1 month after the first presentation at our outpatient clinic. Laboratory tests showed only an elevated white cell count (16 x 109/L) and elevated CRP levels (16× upper normal limit). Procalcitonin and serum aminotransferases were normal. Stool culture and parasitological examinations were negative. Brain MRI and neurological evaluation were normal. Upper gastrointestinal endoscopy was repeated by an experienced endoscopist with a Pentax gastroscope 2990i. The examination was evaluated under white light, without magnification, chromoendoscopy or narrow-band imaging. The oesophageal and gastric mucosa appeared normal. The duodenal mucosa was mildly oedematous, with slight irregularities between the folds (figure 1), but no biopsies were performed. An entero CT scan showed a normal canalisation and no dilatation or small bowel strictures. The patient’s psychiatric evaluation confirmed mild depression; the psychiatrist changed trazodone with haloperidol on account of a reported association between trazodone and vomiting.8
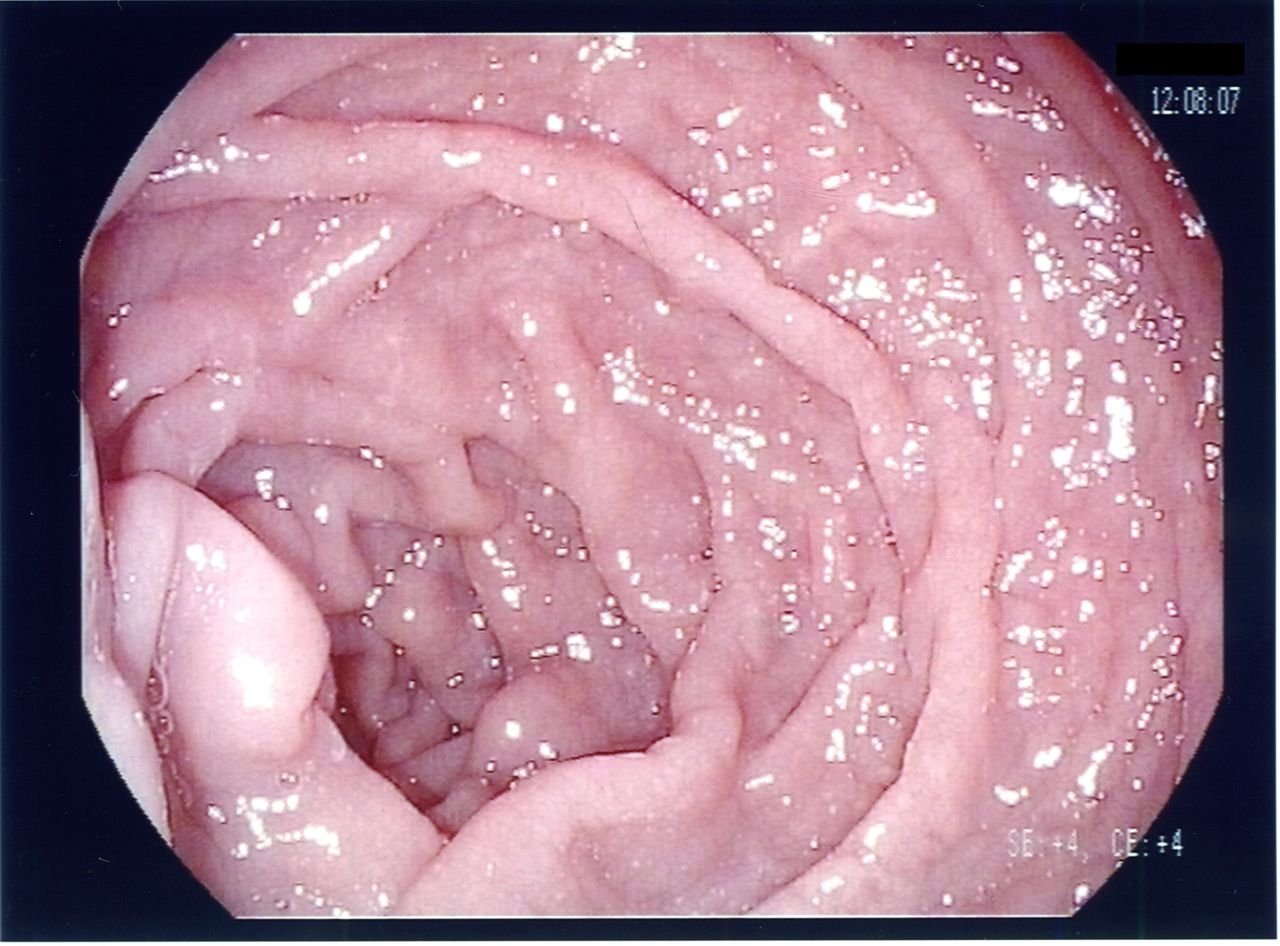
Upper gastrointestinal endoscopy showing oedematous duodenal mucosa with slight irregularities between the folds.
During hospitalisation, the patient was treated with ciprofloxacin 500 mg two times per day and metronidazole 500 mg three times a day on suspicion of an overlapping infectious gastroenteritis. Vomiting episodes disappeared and bowel movements normalised, so she was discharged and her follow-up continued as an outpatient.
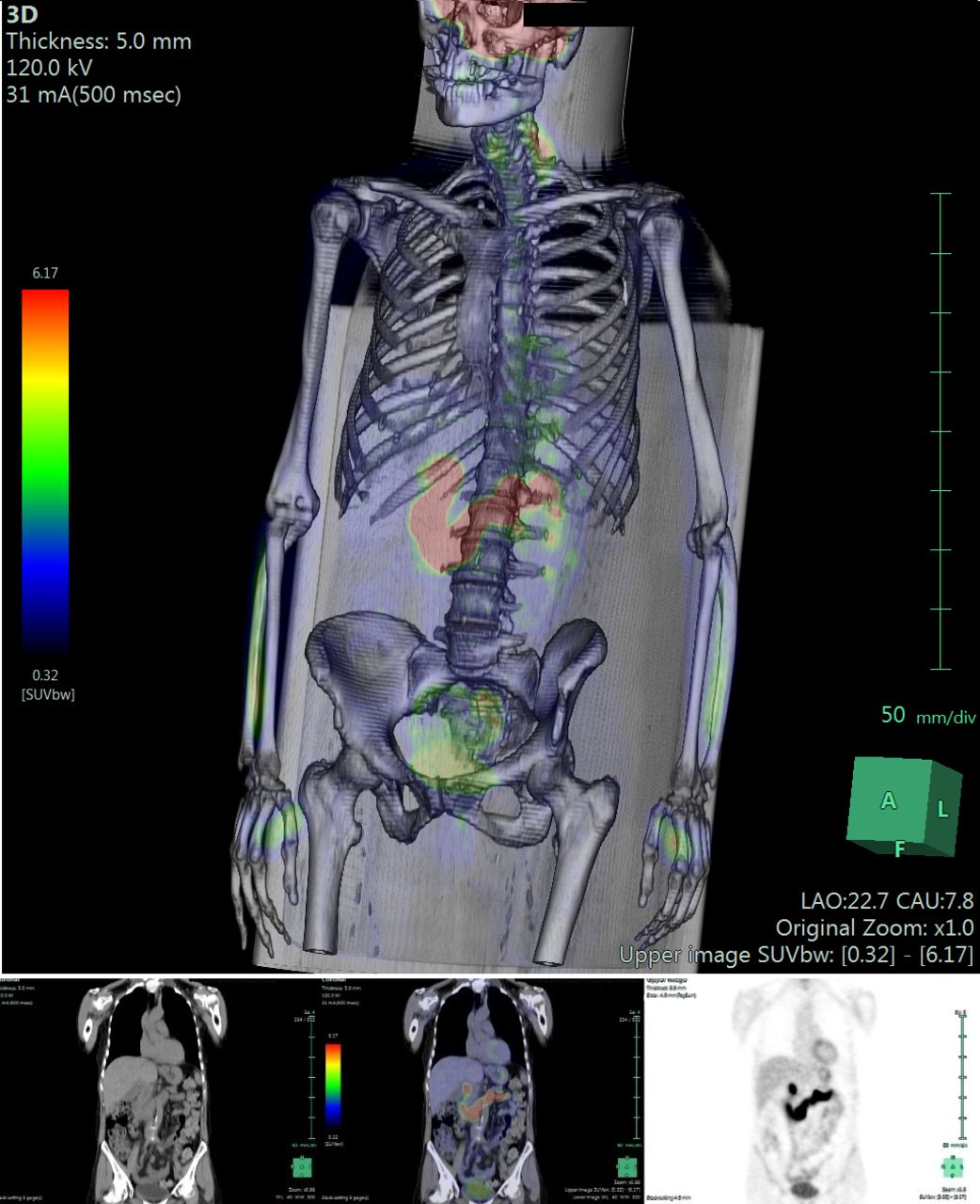
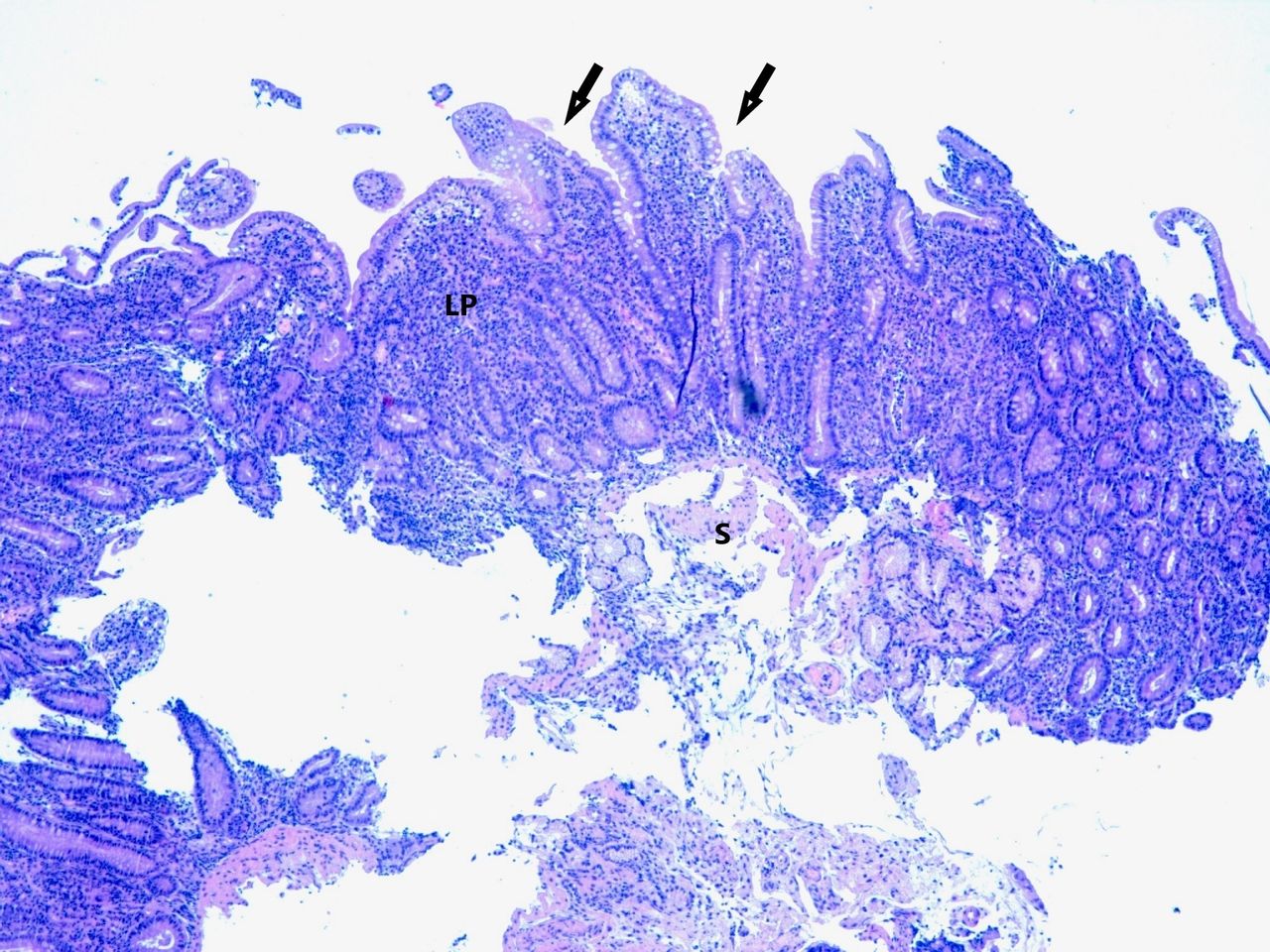
One month later, the patient presented at the emergency department with worsening vomiting, diarrhoea and further 2 kg weight loss. She was hospitalised in the internal medicine department, where the symptoms were attributed to a side effect of canakinumab, which was withdrawn at discharge. However, symptoms continued unchanged. On suspicion of an unrecognised neoplasia, fluorodeoxyglucose positron emission tomography (2-(18FDG)-PET)/CT was prescribed. High-to-moderate uptake (SUVmax 29) of radio-labelled glucose analogue was observed in the duodenum, the first jejunal loop and in the distal jejunum, where areas of fainter uptake suggested the shedding of activated neutrophils inside the lumen of the small intestine (figure 2). The patient was hospitalised again in our gastrointestinal unit. Laboratory tests showed a raised level of serum aminotransferases (5× upper normal limit) and gamma-glutamyl transferase (8× upper normal limit), increased lipase (10× upper normal limit), reduced faecal elastase (52 µg/g, reference range >200 µg/g) and high faecal calprotectin (>1000 mg/kg, reference range <50 mg/kg). Upper gastrointestinal endoscopy was repeated and multiple duodenal biopsies were performed. Histological examination revealed moderate-to-severe hypotrophy of villi (villus crypt ratio 1:1), neutrophilic infiltrate among duodenal enterocytes, with glandular aggression, intraepithelial lymphocytes <25/100, enterocytes and severe chronic lymphoplasmacellular infiltrate of lamina propria (figures 3–5). Congo red staining was negative. Endoscopic ultrasound showed a quite thickened duodenal wall (6.1 mm).
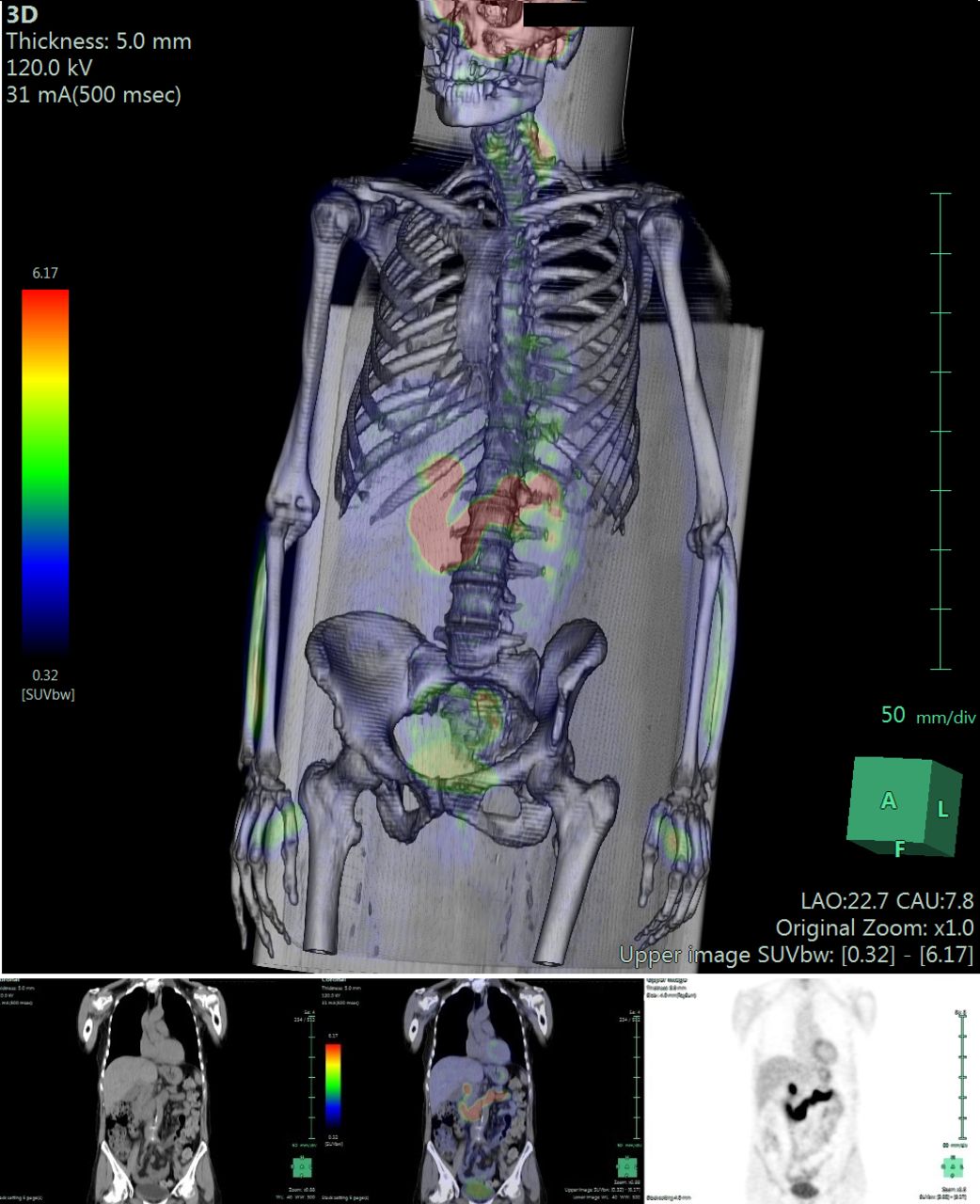
Fluorodeoxyglucose total-body positron emission tomography (PET)/CT showing intense uptake of duodenum, first jejunal loop (SUVmax 29) and distal ileum. Upper panel: three-dimensional reconstruction; lower panel: coronal view of CT, PET/CT and PET.
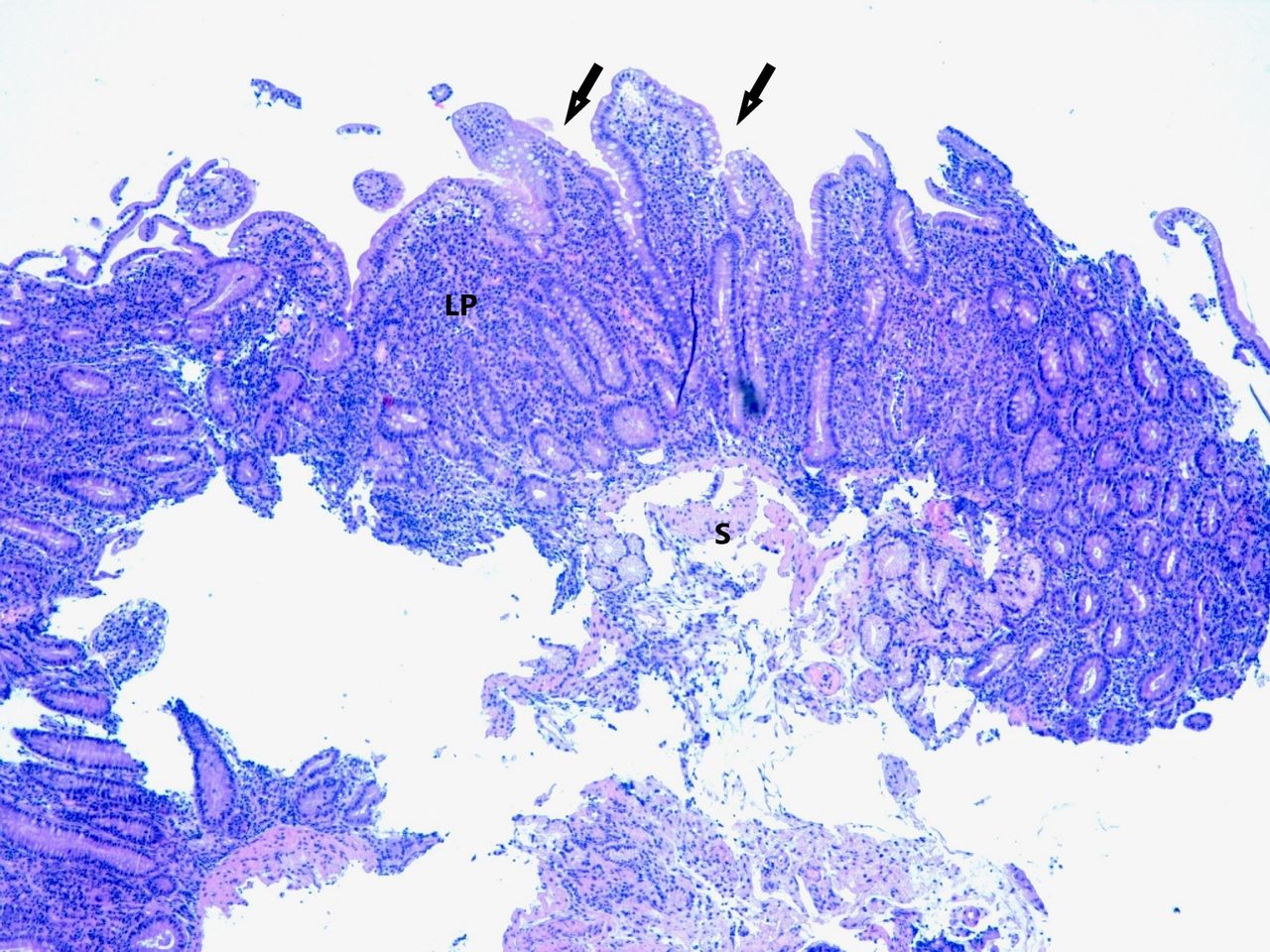
Histological examination with H&E stain showing moderate hypotrophy of villi (arrows), with inflammatory infiltrate in the lamina propria (LP). S, submucosa.

Neutrophilic infiltrate (arrows) among enterocytes (E) and glandular epithelium (G).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
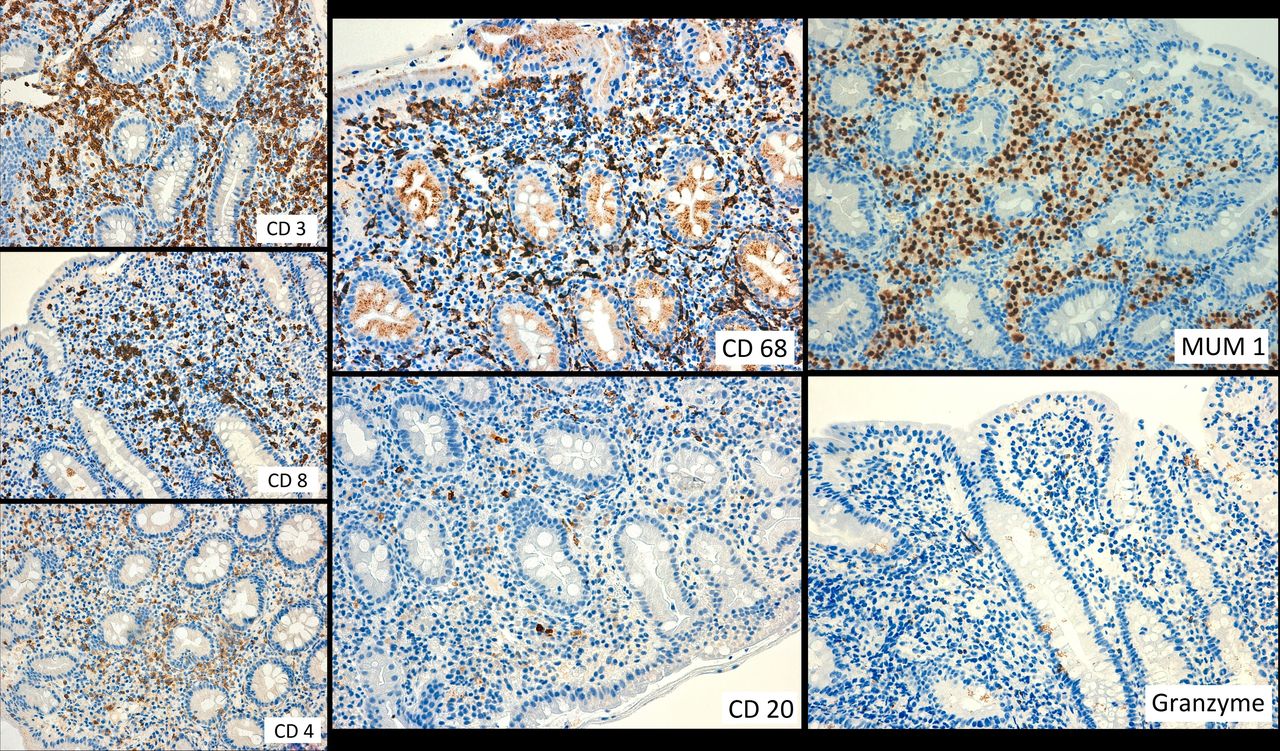
Immunohistochemistry showing severe chronic infiltrate (T and B lymphocytes, plasma cells, macrophages) of the lamina propria without prevalence of any single inflammatory cell type. Intraepithelial lymphocytes were absent. These characteristics exclude coeliac disease, autoimmunity and malignancy. CD3+: T lymphocyte; CD4+: T helper lymphocytes; CD8+: T cytotoxic lymphocytes; CD68+: macrophages; CD20+: B lymphocytes; MUM1+: plasma cells; granzyme+: activated natural killer cells.
Differential diagnosis
Absence of erosions, ulcers and H. pylori infection excluded peptic disease. Clinical history and investigations ruled out all known causes of chronic vomiting9 and microscopic duodenitis.10 Mechanical obstruction was excluded by normal CT enterography. Any side effect of canakinumab was excluded by the lack of clinical improvement after drug withdrawal. Central and psychiatric vomiting was excluded by normal brain MRI, neurological and psychiatric evaluation. Metabolic (diabetes) and endocrine causes (thyroid dysfunction, pregnancy, adrenal insufficiency) were excluded by clinical history, laboratory tests and physical examination. Coeliac disease was ruled out by absent anti-transglutaminase antibodies and normal intraepithelial lymphocytes in duodenal histology. Crohn’s disease was excluded by absence of ulcers and of typical histological patterns. Also, the histological duodenal features were not suggestive of autoimmune enteropathy (plasma cellular infiltrate below normal range), amyloidosis (Congo red negative) and parasitic/infectious diseases (absence of Giardia lamblia and other infectious pathogens). CT enterography, endoscopy and 2-(18FDG)-PET/CT excluded local and distant malignancies.
According to these findings, the duodenojejunal inflammation was attributed to unreported enteric involvement by AOSD. To support this working hypothesis, we planned for strict follow-up of the patient after optimisation of AOSD treatment.
Treatment
Prednisone 50 mg per day was administered over a 4-week period followed by tapering and adalimumab 40 mg every 2 weeks after a charge dose of 160 mg at week 0 and 80 mg at week 2.
Outcome and follow-up
During therapy with high-dose steroids, the vomiting disappeared and the patient gained 2 kg weight. After steroid tapering at 20 mg dosage per day, the patient reported a new onset of vomiting and abdominal pain. Thus, therapy with adalimumab was started and followed by persistent remission of vomiting after some weeks. Four months after the start of biological therapy, laboratory tests showed normal white cell count, a slight increase in transaminases and pancreatic enzymes, normal ferritin, normal faecal elastase and a striking reduction of faecal calprotectin (182 mg/kg). According to these findings, a prominent decrease of radiotracer uptake in the aforementioned intestinal sites was also observed (SUVmax 7.8) at 2-(18FDG)-PET/CT.
Eight months after the start of biological therapy, the patient was found asymptomatic, with normal faecal calprotectin, white cell count, CRP and transaminases. Duodenal histology results improved, with meaningful reduction of inflammatory infiltrate, both neutrophilic and lymphoplasmacellular, and better villi trophysm (1:2).
The patient is now in maintenance therapy on low-dose steroids (prednisone 10 mg daily) and adalimumab 40 mg every other week, and she is clinically stable with no more vomiting.
Discussion
To our knowledge, this is the first reported case of chronic vomiting caused by duodenojejunal inflammation in a woman with AOSD. The duodenojejunal inflammation was revealed by the slightly abnormal appearance of the duodenal mucosa at upper endoscopy, high uptake of 2-(18F)FDG in the duodenum and first jejunal loops at PET/CT scan, strikingly elevated levels of faecal calprotectin and neutrophilic infiltrate among the enterocytes with glandular aggression at histology.
The presence of small bowel inflammation in patients affected by AOSD has previously been reported in a few cases in association with Crohn’s disease, coeliac disease and chronic intestinal pseudo-obstruction.2–7 The association between AOSD and raised intraepithelial lymphocytes11 or between juvenile idiopathic arthritis (the juvenile counterpart of AOSD) and the presence of activated natural killer lymphocytes in the bowel wall12 has also been described. Moreover, a pathogenetic role of the gut immune system in spondyloarthropathies has been hypothesised.13 14 However, the primary involvement of the small bowel with the characteristics described in our patient has not been reported in patients with AOSD until now.
AOSD treatment (high-dose steroids and adalimumab) induced a striking improvement of both vomiting and duodenitis (as confirmed by the decrease of radiotracer in the duodenum and jejunal loops), suggesting a possible causal relationship between the small bowel inflammation and the symptom. The possibility that inflammatory duodenal infiltrate might alter the gastroduodenal motor function has previously been reported in coeliac disease, where the direct impairment of the smooth muscle function, as induced by mucosal inflammation caused by gluten exposition, has been proposed.15 In patients with functional dyspepsia, the duodenal eosinophilic infiltration due to food allergen exposition is supposedly involved in the activation of duodenogastric reflexes underlying an altered gastroduodenal motor function.16 Our case shows that neutrophilic infiltrate might also impair the gastroduodenal motor function and it suggests that duodenal biopsies are potentially useful in case of unexplained gastroduodenal motor dysfunction associated with severe dyspepsia or chronic vomiting. In this context, a functional imaging tool such as 2-(18FDG)-PET/CT potentially supports the clinical suspicion, guides biopsy and monitors disease activity.
Other gastrointestinal manifestations of AOSD in our patient included diarrhoea, increased transaminases, raised levels of pancreatic enzymes and cholestatic indexes, which also improved after biological therapy, thus suggesting a possible relationship with AOSD activity.
Why vomiting in patients with AOSD has never been previously reported remains an intriguing question. Whether the treatment with canakinumab has possibly played a triggering role remains a hypothesis, since vomiting has been mentioned among the side effects of the drug.17 18 However, in partial contrast with this hypothesis, the symptom did not improve when the treatment was stopped.
In conclusion, this case suggests that faecal calprotectin and duodenal biopsies may be useful in patients with AOSD presenting with chronic vomiting, in order to assess the presence of any duodenojejunal inflammation that possibly causes the symptom and resolves after specific anti-inflammatory treatment.
Learning points
Adult-onset Still’s disease (AOSD) may involve the small bowel, presenting with chronic vomiting associated with duodenojejunal inflammation.
Duodenal biopsies might reveal inflammatory causes of gastroduodenal motor dysfunction.
Chronic vomiting in patients with AOSD with duodenojejunal inflammation is potentially favourably treated with immunomodulant therapies.
Ethics statements
Patient consent for publication
Acknowledgments
We thank Dr Marco Maggioni and Professor Stefano Ferrero for the histological examination.
References
Footnotes
Contributors CM cared for the patient and took clinical decisions, designed the work, drafted the work and gave final approval of the version to be published. GB cared for the patient and took clinical decisions, designed the work, drafted the work and gave final approval of the version to be published. AM cared for the patient and took clinical decisions, added specialty details (rheumatology), critically revised the work and gave final approval of the version to be published. MC cared for the patient, added specialty details (nuclear medicine), critically revised the work and gave final approval of the version to be published.
Funding This study was partially funded by Italy’s Ministry of Health and a research grant from Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico (award/grant no. CRUI25OAUNIMI).
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.