Article Text

Statistics from Altmetric.com
Description
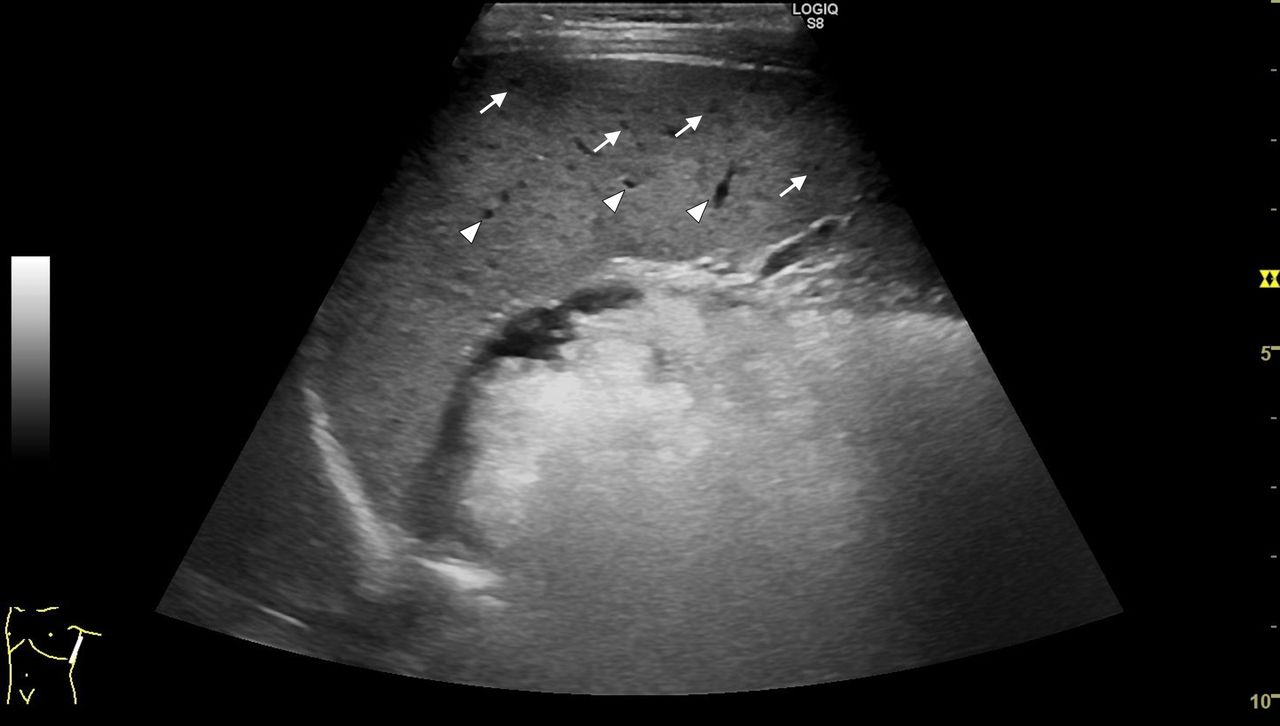
A girl in early adolescence was referred to our facility by a local community hospital with a fever of unknown origin (FUO). She presented with a prolonged fever (10 days) and no other clinical symptoms. The local hospital provided results of abdominal and cardiac ultrasound imaging, head CT and chest radiography, all of which were unremarkable. Blood analysis performed by the local hospital showed leucocytosis and high serum C reactive protein (CRP) level. A thorough clinical history revealed that the patient had fed a stray cat in her yard, and that it had scratched her approximately 2 weeks prior to the onset of the fever. A repeat abdominal ultrasound was performed in our hospital. The ultrasound examination, when performed using an 8.5 MHz high-frequency linear probe, revealed multiple hypoechoic lesions in the spleen (figure 1); however, these were not evident when a standard 3 MHz convex probe was used (figure 2). Further findings included a white cell count of 7.0×109/L (neutrophils, 40.5%), CRP level of 46.4 mg/L and erythrocyte sedimentation rate of 66 mm/hour. A positive serology test for Bartonella henselae confirmed the diagnosis of cat-scratch disease (CSD), and the patient was successfully treated with doxycycline.

8.5 MHz high-frequency linear probe. Arrows show micro-abscesses while arrowheads indicate splenic vasculatures.

{kind=link}
{kind=link}
Standard 3 MHz convex probe.
CSD is a common zoonotic disease among children that is caused by B. henselae. Following inoculation by B. henselae, CSD typically presents with localised lymphadenitis. However, patients may have a systemic clinical manifestation with prolonged fever and micro-abscesses in the liver and/or spleen.1 In a prospective study of 146 children with FUO, CSD was the third most common infectious cause, accounting for seven (4.8%) cases.2 Another study showed organ involvement (liver and spleen) in 35 (8%) out of 437 paediatric CSD hospital admissions.3 Thus, CSD should always be included in the differential diagnoses for children with prolonged fever, and investigation for liver and spleen lesions is critical. Although CT scans or MRI may help detect hepatosplenic lesions in adult patients,4 radiation exposure is a concern in paediatric patients, and children usually require sedation for MRI. Thus, ultrasound screening should be a priority in children, especially those with a history of exposure to a cat. Abnormal findings on abdominal ultrasound in paediatric CSD are common, and according to a previous study, abdominal ultrasound findings showed that 82.4% of these patients had splenic granulomas.5 However, as demonstrated in this case, hypoechoic lesions may be missed if a standard convex probe is used for children because of their smaller body size. Thus, if available, a high-frequency linear probe should be used to screen for splenic lesions.
Patient’s perspective
Patient’s father: It was great to have the cause of my daughter’s fever discovered using ultrasound imaging.
Learning points
Cat-scratch disease (CSD) should be included in the differential diagnoses for fevers of unknown origin. Ultrasound can be used for diagnostic imaging to avoid unnecessary radiation exposure from CT scans and sedation risk with MRI.
Visceral organ involvement is a rare, but important, manifestation of CSD.
A standard convex probe may miss small lesions in children; therefore, a high-frequency ultrasound probe should be used to screen for hypoechoic lesions in the spleen.
Ethics statements
Patient consent for publication
Footnotes
Contributors TT contributed to drafting of the work, data acquisition and analysis of the case for the work. KK contributed to revising the work critically for important intellectual content and final approval of the version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.