Article Text

Statistics from Altmetric.com
Description
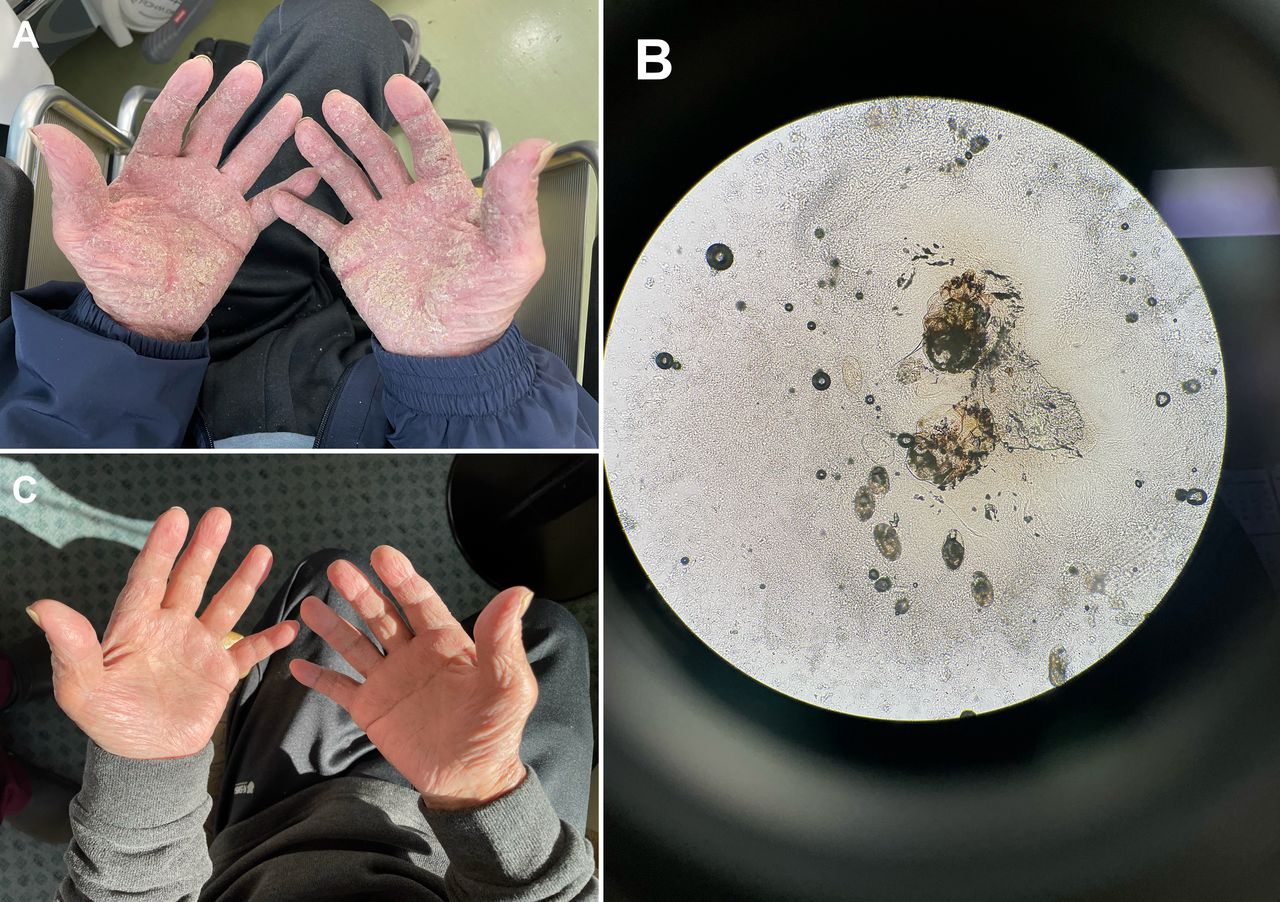
A man in his 70s, with mild cognitive impairment, presented with a 6-month history of a pruritic rash. He had been diagnosed with hyperkeratotic eczema and treated with hydrocortisone butyrate 0.1% (moderate potency) cream 3 months previously. Physical examination revealed dry crusts on his neck, trunk, arms, legs, palms and soles (figure 1A). Microscopy of scrapings of palmar papules revealed scabies mites and eggs (figure 1B). Laboratory testing revealed marked eosinophilia (3645 cells/µL; normal: <500 cells/µL). The patient was diagnosed with crusted scabies. He was hospitalised and treated with oral ivermectin 200 µg/kg on days 1 and 8, crotamiton 10% cream and phenothrin 5% lotion. His eosinophil count normalised after 1 week; however, it increased again 2 weeks later. Microscopy of scrapings from crusted sole papules revealed mites and eggs. Ivermectin was repeated six times. The rash subsided 4 weeks after treatment initiation (figure 1C). The patient’s family members were treated with oral ivermectin and crotamiton 10% cream; all bedsheets and clothes were cleaned, and he was discharged home.

{kind=link}
Findings of crusted scabies. (A) Dry crusts on the patient’s palms on presentation. (B) Microscopy of skin scrapings of palmar papules showing scabies mites and eggs. (C) The patient’s palms 4 weeks after starting treatment showing clearing of the rash.
Crusted scabies is a severe form of scabies and is highly contagious. In classic scabies, patients have approximately 10–15 mites, whereas patients with crusted scabies can have several thousands.1 The risk of crusted scabies is high in nursing homes and hospitals, and among socially disadvantaged populations and immunocompromised individuals.2 The diagnosis might have been missed by the first physician because the patient did not describe his symptoms clearly and an inadequate diagnostic evaluation. Physicians should be knowledgeable about the diagnosis and treatment of scabies, to avoid misdiagnosis and inadequate treatment.
Skin scraping of burrows or erythematous papules should be performed. Mites are easily found in patients with crusted scabies, but negative skin scraping results do not rule out classic scabies because the number of mites may be low. Dermoscopy is helpful for visualising mites and burrows.3 4 Mites can be identified in grey delta structures at the edge of burrows are collected with a small blade and observed under a microscope.
Postscabetic itch, due to the immune response to mite antigens, may persist for several months.5 Dermoscopy and scrapings are important for determining whether the itching is due to residual scabies or an allergic reaction. Postscabetic itch can be treated with oral antihistamines and topical corticosteroids. Persistent infestation may be due to incorrect application and poor penetration of topical treatment through crusted skin, reinfestation or drug-resistant mites.6 Most recurrences are caused by reinfestation from untreated contacts,7 so family members and close contacts should be treated, regardless of whether they are symptomatic. Ivermectin resistance has been reported in individuals with intensive ivermectin exposure8 but is rare in Japan. Oral ivermectin 200 µg/kg on days 1 and 8 is the first-line treatment for crusted scabies. Ivermectin is not ovicidal; thus, two doses are required to kill hatchlings before they breed. Crusted scabies is refractory to initial treatment because of the large number of mites and heavy skin crusting.9 Therefore, repeated ivermectin administration may be necessary if ova are still present after two doses, as in this case.
Learning points
Cases of crusted scabies may require more than two doses of ivermectin, administered 1 week apart.
Most recurrences are caused by reinfestation from untreated contacts; therefore, contacts must be treated simultaneously.
Dermoscopy and skin scrapings are important for determining whether itching is due to residual scabies or an allergic reaction.
Ethics statements
Patient consent for publication
Acknowledgments
The authors wish to thank Satoru Arai, Department of Dermatology, St Luke’s International Hospital, Tokyo, Japan, for his professional support. We also wish to thank Iroha Yamamoto, Junior Resident, St Luke’s International Hospital, Tokyo, Japan, for her kind support. We would like to thank Editage (www.editage.com) for English language editing.
Footnotes
Contributors TN, KI, MT cared the patient and wrote the report. HA read and approved the final version of the report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.