Article Text

Statistics from Altmetric.com
Description
We describe a male patient in his 50s, who underwent bilateral lung transplantation for end-stage disease secondary to pulmonary sarcoidosis. His preoperative total lung capacity (TLC) was calculated at 3.94 L (53% predicted) on plethysmography. The donor’s predicted TLC was estimated at 4.39 L. Intraoperatively an abundance of extrapericardial adipose tissue was encountered consistent with preoperative imaging (figure 1); once both lungs had been implanted, it became apparent that bilateral upper lobe expansion would be suboptimal due to the bulk of adipose tissue attached to the outer surface of the pericardium.

The abundance of extrapericardial adipose tissue outlined in this CT tilted coronal view.
Once this was meticulously excised (in excess of 500 g), the upper lobes expanded to their anatomical position in the recipient’s chest (figure 2). We did allow for a further 48 hours prior to formal chest closure by approximation of the skin with incorporation of a small Bogota bag within the middle aspect of the wound.
{kind=link}
{kind=link}
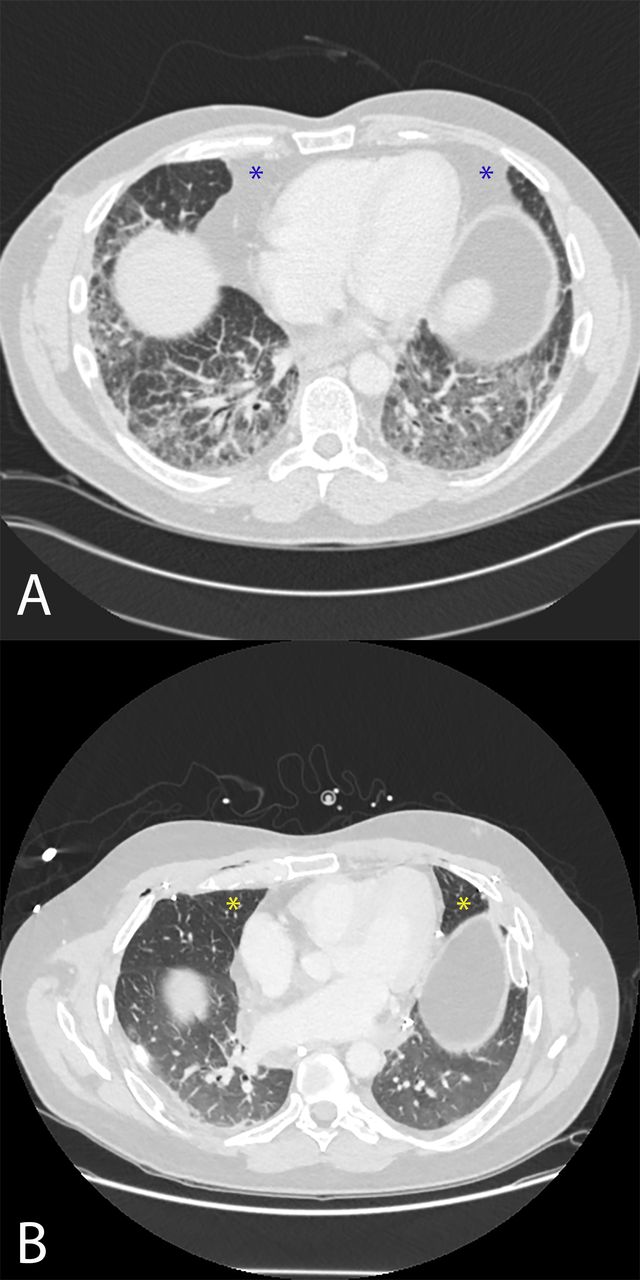
Preoperative (A) and postoperative (B) CT axial images are shown for comparison. Whereas the pericardiophrenic recesses are occupied by adipose tissue in the former (blue asterisks), the upper lobes fill these spaces postoperatively (yellow asterisks).
Although oversizing of pulmonary allografts has been associated with improved survival especially in the context of bilateral lung transplantation without increasing post-transplant complications,1 2 oversizing can lead to a variety of undesirable complications including perpetual atelectasis, distortion of bronchial anatomy with retention of secretions and increased risk for secondary infection.3 A variety of surgical procedures including split lung transplantation, lobar transplantation and peripheral segmental resection are used to permit larger lungs to be downsized for use in smaller recipients.3 Surgical manipulation of pulmonary allografts at the back-table prior to transplantation or post-transplantation predispose to several complications including bronchial anastomotic issues, prolonged air leak and pleural space contamination.
Delayed chest closure is a technique used to avoid thoracic compartment syndrome causing haemodynamic instability and desaturation. It is commonly used in damage control surgery for thoracic trauma.4 A variety of approaches exist spanning from Esmarch bandaging, Bogota bag, simple skin closure with or without active thoracic cage splinting or intrathoracic gauge packing. Indications for delayed chest closure in transplantation include acute lung oedema, oversize allograft, coagulopathy, haemodynamic instability or impaired arterial partial pressure of O2/ Fraction of inspired O2 ratio (PaO2/FiO2).5 With appropriate medical management including extracorporeal membrane oxygenation if indicated, the chest can be formally closed within a few days.
A variety of terms is used to describe the adipose tissue situated on the external surface of the parietal pericardium within the literature, including extrapericardial, paracardial, mediastinal and intrathoracic.6 7 Resection of excess adipose tissue attached to the pericardium appears to be a useful adjunct to avoid allograft volume reduction with associated complications.
Learning points
Oversizing of pulmonary allografts has been associated with improved survival without increasing post-transplant complications.
Resection of excess adipose tissue attached to the pericardium may be useful as an adjunct to avoid allograft volume reduction.
Ethics statements
Patient consent for publication
Footnotes
Contributors ID performed the operation and was responsible for the concept of the procedure. BHNC was responsible for the writing and the collation of the figures as well as the submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.