Article Text

Statistics from Altmetric.com
Description
Introduction
We present a case of a middle-aged man with symptoms and signs of hyperthyroidism. Technetium-99 thyroid scan was suggestive of Marine-Lenhart syndrome, a rare entity. It must be treated promptly and carefully given the possibility of an incorrect diagnosis. Thus, assessing the functional status of nodules in Grave’s disease is of utmost importance in reducing the morbidity and mortality associated with Marine-Lenhart syndrome.
Case report
A previously healthy middle-aged man presented with a 2-week history of palpitations, excessive sweating and a 5 kg weight loss. On examination, he was tachycardic, had tremors of the upper extremities and diffuse goitre. Eye signs like proptosis and lid lag were absent. Cardiovascular and respiratory examination revealed no abnormalities. His initial laboratory investigations revealed a suppressed thyroid-stimulating hormone (<0.005 μIU/mL), high free thyroxine levels (4.58 ng/dL). Complete blood counts, blood sugars and renal and liver functions were normal.
Technetium-99 thyroid scan showed diffuse enlargement of both lobes of the thyroid gland along with focal increase in radiotracer uptake in the mid zone of right lobe. A focal photopenic area was also noted in the mid zone of left lobe. The rest of the thyroid gland slowed diffusely increased radiotracer uptake (figure 1). All these scan findings were suggestive of diffuse thyroid goitre (Graves’) with autonomous functional thyroid nodules (AFTN) in the right lobe—Marine-Lenhart syndrome. A cold nodule was noted in the left lobe, warrantingultrasonography (USG)-guided Fine Needle Aspiration Cytology (FNAC).

Technetium 99 thyroid scan showing diffuse enlargement of both lobes of the thyroid gland along with focal increase in radiotracer uptake in the mid zone of right lobe. Focal photopenic area also noted in the mid zone of left lobe. Rest of the thyroid gland shows diffusely increased radiotracer uptake. (A): Anterior, (B: Right anterior oblique, C: Left anterior oblique.
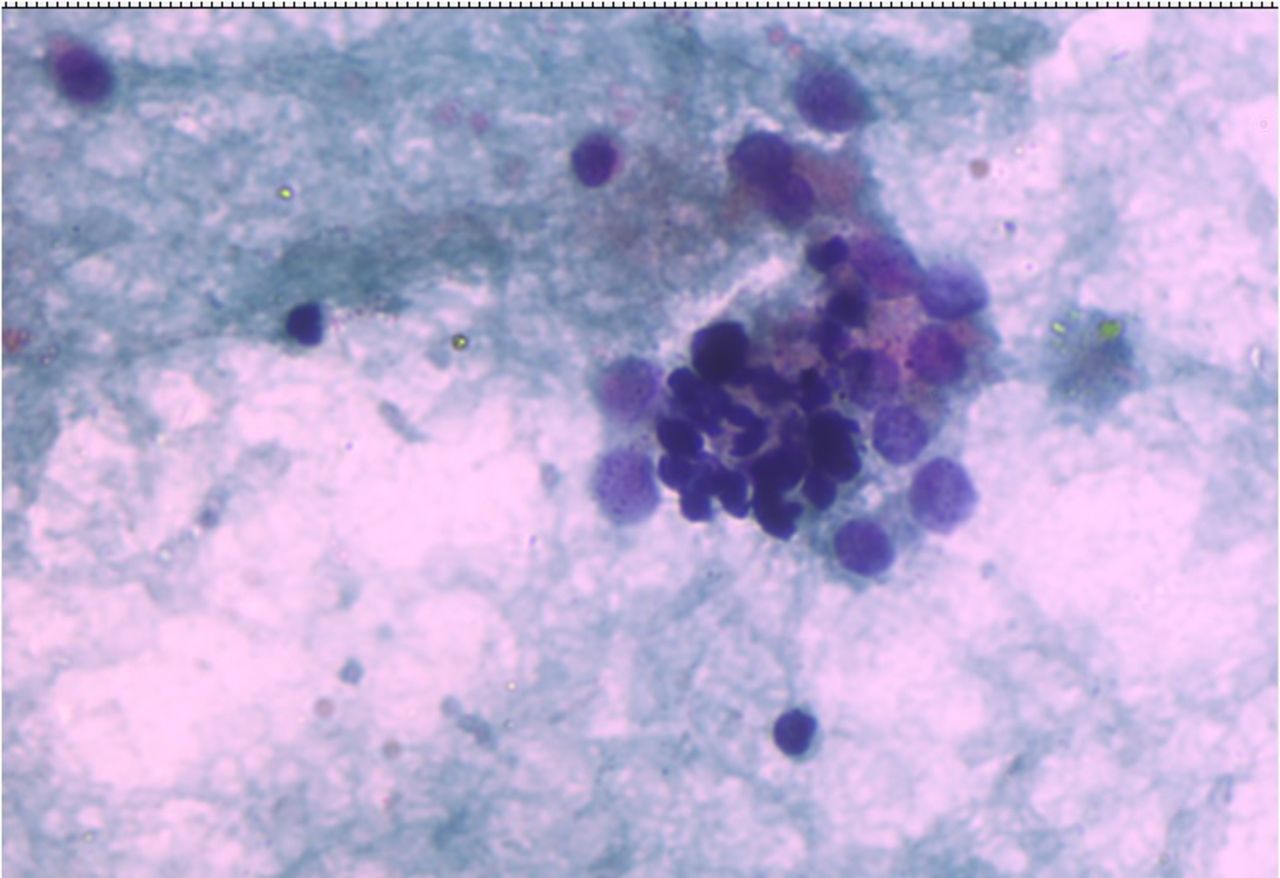
Cytology showed monolayered clusters and microfollicles and single benign thyroid cells showing enlarged nuclei, nuclear overlapping, anisonucleosis, granular chromatin, multiple nucleoli and occasional ones showing nuclear grooves with vacuolated cytoplasm along with few scattered hurthlised cells, lymphocytes and hemosiderin-laden macrophages in a background of thin colloid and haemorrhage (figures 2 and 3). These findings once again pointed towards possibility of Graves with adenomatous nodule in Goitre (Bethesda System for Reporting Thyroid Cytopathology (BSRTC) category 2).

Fine Needle Aspiration Cytology (FNAC) thyroid shows monolayered clusters of follicular cells against a background of colloid and macrophages, suggestive of Colloid goitre, 100×, Papanicolou stain.

{kind=link}
{kind=link}
{kind=link}
Smear shows clusters of follicular cells with abundant pale cytoplasm, enlarged nuclei and infiltrated by lymphocytes, suggesting possibility of Graves’s disease. 200×, Papanicolou stain.
The patient was informed in detail about all possible treatment options (radioiodine therapy, antithyroid drugs and surgery). Radioiodine therapy has the advantage of permanent resolution of the disease; however, a greater dose is necessary in Marine-Lenhart syndrome (MLS).1 Surgery also provides a permanent cure, however, there are risks of permanent hypothyroidism, iatrogenic hypoparathyroidism and recurrent laryngeal nerve damage. Thionamides, on the other hand, hardly allow remission of the disease but have lower initial costs making them a common choice in developing countries. The patient chose antithyroid drugs and was started on carbimazole 10 mg two times per day and propranolol 20 mg two times per day following which his symptoms improved.
Discussion
Marine-Lenhart syndrome is defined as the coexistence of Graves’ disease and AFTN.1 The syndrome is quite rare, estimated to occur in around 0.8%–2.7% of patients with Graves’ disease.2
Some cases that had developed Graves’ disease after radiotherapy for AFTN were inappropriately included in this syndrome, thus scintigraphy and autoimmune testing are paramount in establishing the diagnosis. The pathophysiology of this syndrome includes the release of thyroid hormones from AFTN tissues the can be accelerated in response to TSH‐receptor stimulation.3
If oral antithyroid therapy is chosen as first-line treatment for Graves’, missed active nodules may result in failure of achievement of euthyroidism. Furthermore, if radioactive iodine therapy is chosen for treatment of Marine-Lenhart syndrome, the given radioactive iodine dose may not be enough as these patients are relatively radioiodine resistant, requiring higher activities of I- 131.4
In cases involving multiple hot nodules, surgical intervention may be more appropriate as these patients require a higher dose of radioactive iodine for successful treatment. Also, finding a cure with oral antithyroid therapy is not possible when considered from a pathophysiological point of view.
In our patient’s case, since he had a single hot nodule, oral antithyroid therapy alone resulted in cure.
In conclusion, physicians must be careful in interpreting thyroid scans in Graves’ disease. If the existence of thyroid nodules is confirmed, their activity must be determined with further evaluation, to make an optimal treatment choice in time.
Learning points
Marine-Lenhart syndrome is a rare disease occurring in patients with Graves’ disease.
Functional status of nodules (hot/cold) discovered in Graves’ disease must be determined to rule out malignancy.
In case of radioactive iodine therapy, a higher dose is necessary to treat patients with Marine-Lenhart syndrome, as compared with those with Graves’ disease.
Presence of multiple autonomous hot nodules necessitates surgical treatment.
Ethics statements
Patient consent for publication
Footnotes
Contributors BBK, AMM, SSM, SPM: conception and design, acquisition of data or analysis and interpretation of data; drafting the article or revising it critically for important intellectual content; final approval of the version published. KP: involved in histopathological diagnosis and provided thyroid FNAC photomicrographs.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.