Article Text

Abstract
A man in his 50s presented with persistent chest pain, haemoptysis, cough and dyspnoea 5 months after undergoing catheter ablation for atrial fibrillation (AF). Several chest CT scans suggested pneumonia. Despite adequate treatment for recurrent pneumonia, symptoms persisted. While reviewing the initial chest CT, a partial venous infarction of the left lower lobe associated with severe left inferior pulmonary vein stenosis (PVS) was diagnosed. Stenting of the left inferior pulmonary vein with a vascular bare metal stent was performed, guided by fluoroscopy and transoesophageal echocardiography. Dual antiplatelet therapy (aspirin/clopidogrel) was introduced for 3 months, followed by long-term aspirin monotherapy. The treatment resulted in relief of his symptoms and the resolution of pulmonary opacities on chest CT. Despite low frequency, AF ablation remains the most common cause of acquired PVS. As highlighted in this case, symptoms are not specific and include recurrent pulmonary infection with delayed management.
- Arrhythmias
- Interventional cardiology
- Pneumonia (infectious disease)
- Pacing and electrophysiology
- Radiology (diagnostics)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Arrhythmias
- Interventional cardiology
- Pneumonia (infectious disease)
- Pacing and electrophysiology
- Radiology (diagnostics)
Background
Atrial fibrillation (AF) ablation remains the most common cause of acquired pulmonary vein stenosis (PVS), despite a decrease in the frequency of this complication in recent years.1–3 First described in 1998,4 PVS was a common complication of AF ablation with the earliest techniques involving ablation within the pulmonary vein themselves. To avoid this issue, AF ablation techniques further evolved towards more proximal pulmonary vein isolation (circumferential or segmental) by first ostial ablation, and nowadays antral isolation. With this latest technique, the incidence of severe PVS decreased to less than 1%.5 Nowadays, the diagnosis of PVS is often delayed or missed and it should not be forgotten. Here, we report a case of PVS with a delayed diagnosis despite suggestive symptoms.
Case presentation
A man in his 50s was admitted for his third episode of pneumonia in 2 months. His medical history includes a pneumothorax treated conservatively during his 30s, a paroxysmal AF treated by radiofrequency catheter ablation 5 months prior to his presentation, an ophthalmic migraine, and a 20 pack-year history of smoking. During the last few months, the patient developed recurrent respiratory symptoms characterised as chest pain, cough, minor haemoptysis and shortness of breath leading to several medical consultations. Physical examination revealed coarse crackles at the left inferior lobe without signs of respiratory distress.
Investigations
His ECG and routine laboratory tests with D-dimer were initially normal. An inflammatory syndrome (C reactive protein 124 mg/L) was later noticed, with a negative nasopharyngeal SARS-COV2 PCR (PCR). In total, three chest CT scans were performed in 2 months. On the first CT, ground glass opacities of the left inferior lobe suggesting viral pneumonia were found. The second imaging study showed a progression of the ground glass opacities in addition to the development of heterogeneous condensation, suggesting bacterial pneumonia. Despite the introduction of co-amoxicillin, a third CT scan revealed worsening of the opacities, leading to a switch of antibiotics to levofloxacin. Clinical and biological evolution was transiently favourable, but pulmonary symptoms persisted for more than 1 month. A fourth chest CT showed improvement of the condensations but the persistence of ground glass opacities of the left inferior lobe, compatible with a partial venous infarction of the left lower lobe (figure 1). After reviewing the first chest CT scan with contrast, an opacification delay was observed in the left inferior pulmonary vein suggestive of stenosis or thrombotic occlusion (figure 2). A pulmonary CT angiography was performed, showing a residual flow and confirming severe stenosis of the left inferior pulmonary vein without complete occlusion (figure 3). Transoesophageal echocardiography showed a normal ejection fraction and no significant valvulopathy. The mean gradient was measured at 4.3 mm Hg (maximal gradient of 10 mm Hg) in the left inferior pulmonary vein systolodiastolic flow.

Chest CT scan showing ground glass opacities of the left inferior lobe, compatible with a partial venous infarction of the left lower lobe (yellow arrows).

Chest CT scan with contrast showing an opacification delay in the left inferior pulmonary vein (yellow arrow) suggestive of stenosis or thrombotic occlusion.

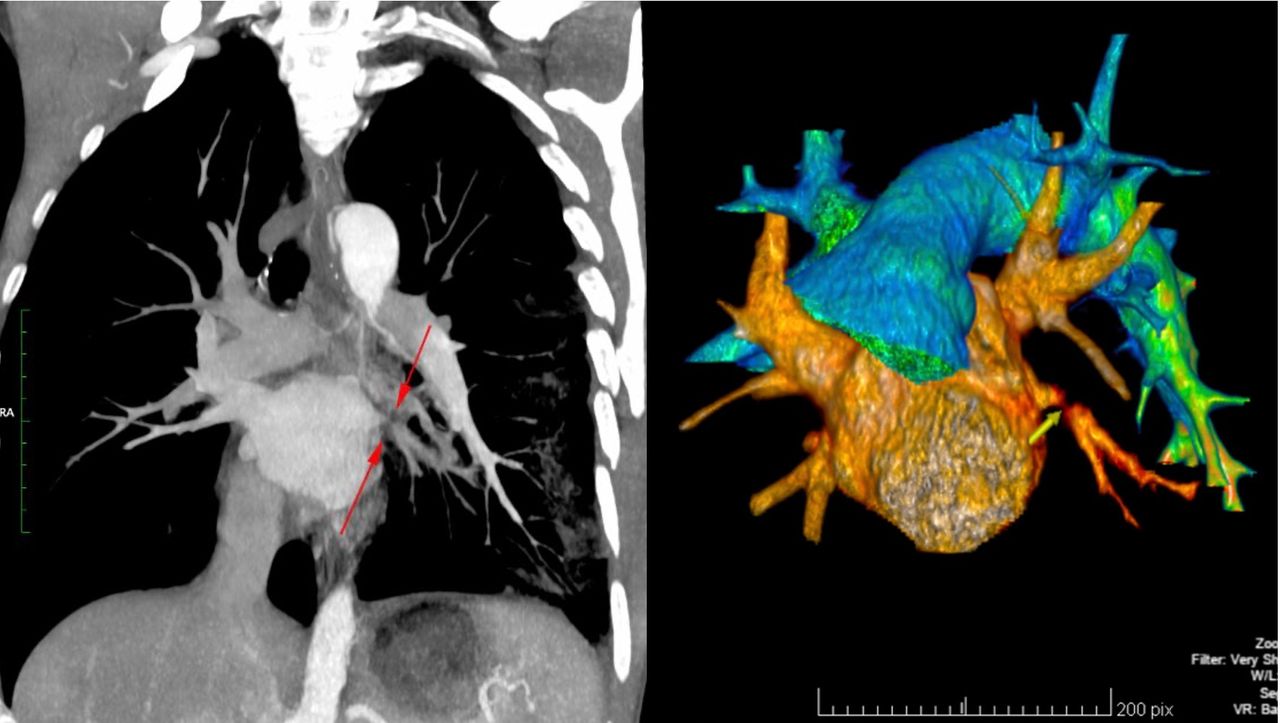
Pulmonary CT angiography showing severe stenosis of the left inferior pulmonary vein without complete occlusion (red arrow on the left figure) and three-dimensional reconstruction (yellow arrow on the right figure).
Treatment
A pulmonary vein angiography was performed under general anaesthesia by way of right femoral veinous access, followed by transseptal puncture and injection of the pulmonary veins. The stenosis of left inferior pulmonary vein was predilated by a 5 mm (EUPHORA 5×15 mm, Medtronic) balloon. A vascular balloon-expandable bare metal stent (over the wire OMNI ELITE 8.0×19 mm, Abbott Vascular) was then implanted from the ostium to above the first bifurcation. The stent was postdilated by an 8 mm (Powerflex PRO 8×40 mm, Cordis) balloon in the distal part and a 10 mm (Powerflex PRO 10×40 mm) balloon in the proximal part of the pulmonary vein. The intervention was guided by fluoroscopy and transoesophageal echocardiography (figure 4). The treatment resulted in a decrease in the mean and maximal gradient of the left inferior pulmonary vein systolodiastolic flow from 4.3 to 2 mm Hg and from 10 to 7 mm Hg, respectively. A 3-month dual antiplatelet therapy with aspirin and clopidogrel was introduced, followed by long-term aspirin monotherapy.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Stenting of left inferior pulmonary vein (LIPV) (A): severe stenosis of LIPV in fluoroscopy (yellow arrow on upper figure) and transoesophageal echocardiography (red arrows on lower figure): LIPV systolodiastolic flow mean gradient 4.3 mm Hg and maximum gradient 10 mm Hg. (B) stenting (Omni elite 8.0×19 mm) of LIPV in fluoroscopy (yellow arrow on upper figure) and transoesophageal echocardiography (red arrows on lower figure). (C) Final result in fluoroscopy (yellow arrows on upper figure) and transoesophageal echocardiography (red arrows on lower figure): left inferior pulmonary vein systolo-diastolic flow mean gradient 2 mm Hg and maximum gradient 7 mm Hg
Outcome and follow-up
After the intervention, the symptoms immediately improved. At 6-month follow-up, the patient had no cardiorespiratory symptoms. A chest CT confirmed stent patency and a near complete resolution of the pulmonary opacities.
Discussion
The presentation of PVS is variable and the symptomatology depends on the severity of the PVS and the number of pulmonary veins affected.6 Symptoms are not specific, including shortness of breath, cough, fatigue, chest pain, haemoptysis and recurrent pulmonary infection, and appear after a mean of 4.0±3.0 months after the most recent ablation procedure.7 The average delay between onset of symptoms and diagnosis of PVS was 4.4±5.4 months in a prospective, observational study that included 124 patients with severe PVS between 2000 and 2014.7 Diagnosis delay can lead to useless or even harmful exams, such as bronchoscopy or pulmonary biopsy. Furthermore, PVS can progress to total occlusion of the pulmonary vein, which would complexify or prevent its treatment.
PVS can be diagnosed by CT or MRI. These modalities help define the severity of PVS, ranging from mild (<50%), moderate (50%–70%) to severe (>70%), depending on the percentage reduction of the luminal diameter according to the 2017 expert consensus.2 Perfusion scans and transoesophageal echocardiography constitute alternative imaging modalities. In addition, pulmonary venography is particularly useful when total occlusion of the pulmonary vein is suspected on CT scan as it may reveal a residual channel allowing the introduction of a catheter for invasive treatment.
Intervention should be considered when the patient is symptomatic. Patients with asymptomatic PVS should be monitored by imaging every 3–6 months and angioplasty should be considered when PVS is severe, especially in presence of ipsilateral PVS.8 The treatment consists of angioplasty of the pulmonary vein and provides a significant improvement of symptoms.9 However, according to a recent meta-analysis, the overall incidence of restenosis remains high, up to 46% at 32 months, but is higher with balloon angioplasty alone (62.0%) compared with stenting (28.5%, risk ratio RR 2.18 (95% CI 1.64 to 2.89), p=0.001), with a comparable safety.10 Some studies suggest that long-term patency could be superior with stent sizes larger than 9 mm in diameter.9 11 Continuing follow-up is therefore recommended.
Conclusion
PVS is a serious complication of AF ablation that can be easily misdiagnosed. Although the incidence of this complication decreased due to technical improvements, it is important to mention the diagnosis of PVS when a patient presents with suggestive symptoms post AF ablation. The longer the diagnosis is delayed, the greater the vascular and parenchymal lung damage, and in turn the more difficult it is to treat the PVS. Currently, the treatment of choice is angioplasty with stenting, preferably with a stent larger than 9 mm in diameter. A successful angioplasty can significantly relieve symptoms.
Patient’s perspective
My story starts with an ablation procedure to treat atrial fibrillation which initially started 7 months prior to the intervention. As part of the standard post-operative medication, I was put on apixaban for 3 months. 2 days after stopping the apixaban I started experiencing severe pain in my left lung, coughing blood. After visiting emergency department I was initially diagnosed with suspected pneumonia and put on a course of antibiotics. After 7 days, and with my condition not improving, I was put on another type of antibiotic. After another 10 days with no progress, I was admitted to hospital again for further scans and tests which revealed a stenosis in one of my pulmonary veins.
Immediately after the procedure to reopen this pulmonary vein with a stent the lung pain and coughing of blood completely stopped. I have not had any reoccurrence of the lung issues since the procedure.
Learning points
Pulmonary vein stenosis (PVS) should be suspected when suggestive symptoms (shortness of breath, cough, fatigue, chest pain, haemoptysis and recurrent pulmonary infection) develop after atrial fibrillation ablation procedure.
Treatment is indicated when symptomatic.
Treatment consists of angioplasty of the pulmonary vein.
The overall incidence of restenosis after angioplasty alone is high, up to 46% at 32 months, but is lower with stenting (especially with stent sizes larger than 9 mm in diameter) compared with balloon angioplasty alone.
Ethics statements
Patient consent for publication
Acknowledgments
We acknowledge the patient for his consent to publish the case. We acknowledge Dr Alix Juillet De Saint Lager for the images. We acknowledge Pr Dipen Shah for his review.
Footnotes
Contributors AM and SN conceived and designed the manuscript. AM collected and analysed the clinical data. AM wrote the original draft. SM-W and HM and SN. revised the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.