Article Text

Abstract
We experienced a case of anterior glottic web with bilateral vocal cord cancers. The laryngoscopic findings showed milky tumour lesions on bilateral vocal cords and a web-like formation with an adhesion in the anterior commissure. In this case, we performed laryngomicrosurgery to remove the bilateral vocal cord tumours and the anterior glottic web. This case was diagnosed as bilateral glottic carcinoma (laryngeal carcinoma TNM classification: pT1bN0M0) with an anterior glottic web. Therefore, this patient underwent radiation therapy (66 Gy). At present, one and a half years have passed since the end of radiotherapy. There is no recurrence of the glottic cancer or web. The airway at the glottis was patent. It has been reported that cutting-off the anterior glottic web could easily lead to readhesion. Accordingly, we continued to follow-up to determine whether there was a recurrence of readhesion of the anterior glottic web or glottic cancer.
- Head and neck surgery
- Head and neck cancer
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
The glottic web can cause dysphonia or dyspnoea due to membrane-like structures between the bilateral vocal cords. This disease is classified as congenital and acquired types. There have been few cases of congenital glottic web, and many were the acquired type.1 2 Holinger3 and Kou4 reported that congenital webs represent <5% of all congenital laryngeal anaomalies. Kou4 recommended that all patients with anterior glottic web should be evaluated for chromosome 22q11.2 deletion syndrome. Acquired cases would be caused by inflammation and damaged vocal cords due to various factors.5–7 Watanabe et al6 reported that many cases with acquired glottic webs involved a postoperative factor (44.7%). Figi7 described cases that did not arise from postoperative causes including infections such as syphilis, tuberculosis, leprosy, blastomycosis, rhinoscleroma and infectious granulomas. There has been no report of a case of glottic web with laryngeal cancers. We experienced a case of anterior glottis web with bilateral vocal cord cancer and present the clinical findings, including histopathological examination, treatments, progress and some consideration of the relevant literature.
Case presentation
A patient was Japanese man in his 60s. His chief complaint was hoarseness 1 month before, but experienced no dyspnoea. He was diagnosed with bilateral vocal cord polyps by a medical practitioner. This practitioner introduced him to our hospital. At the first examination, the laryngoscopic findings showed milky tumour lesions on bilateral vocal cords and a web-like formation with adhesions including anterior commissure (figure 1). The laryngeal lesions were very small and could not be found in the CT scan. Visual palpation, echo and CT scan revealed no cervical lymph node metastasis and no lung metastasis findings. The preoperative diagnosis was anterior glottic web with bilateral vocal cord tumours. The patient underwent laryngomicrosurgery to remove the bilateral vocal cord tumours, and the anterior glottic web was cut-off and removed. On histopathological examination, all of the bilateral vocal cord tumours and the tumour in the anterior glottic web could be observed as squamous cell carcinoma with granulation formations in the background and surrounding invasion (figure 2). The postoperative diagnosis was bilateral glottic carcinoma (laryngeal carcinoma TNM classification: pT1bN0M0) with an anterior glottic web. Therefore, the patient received radiation therapy (66 Gy).
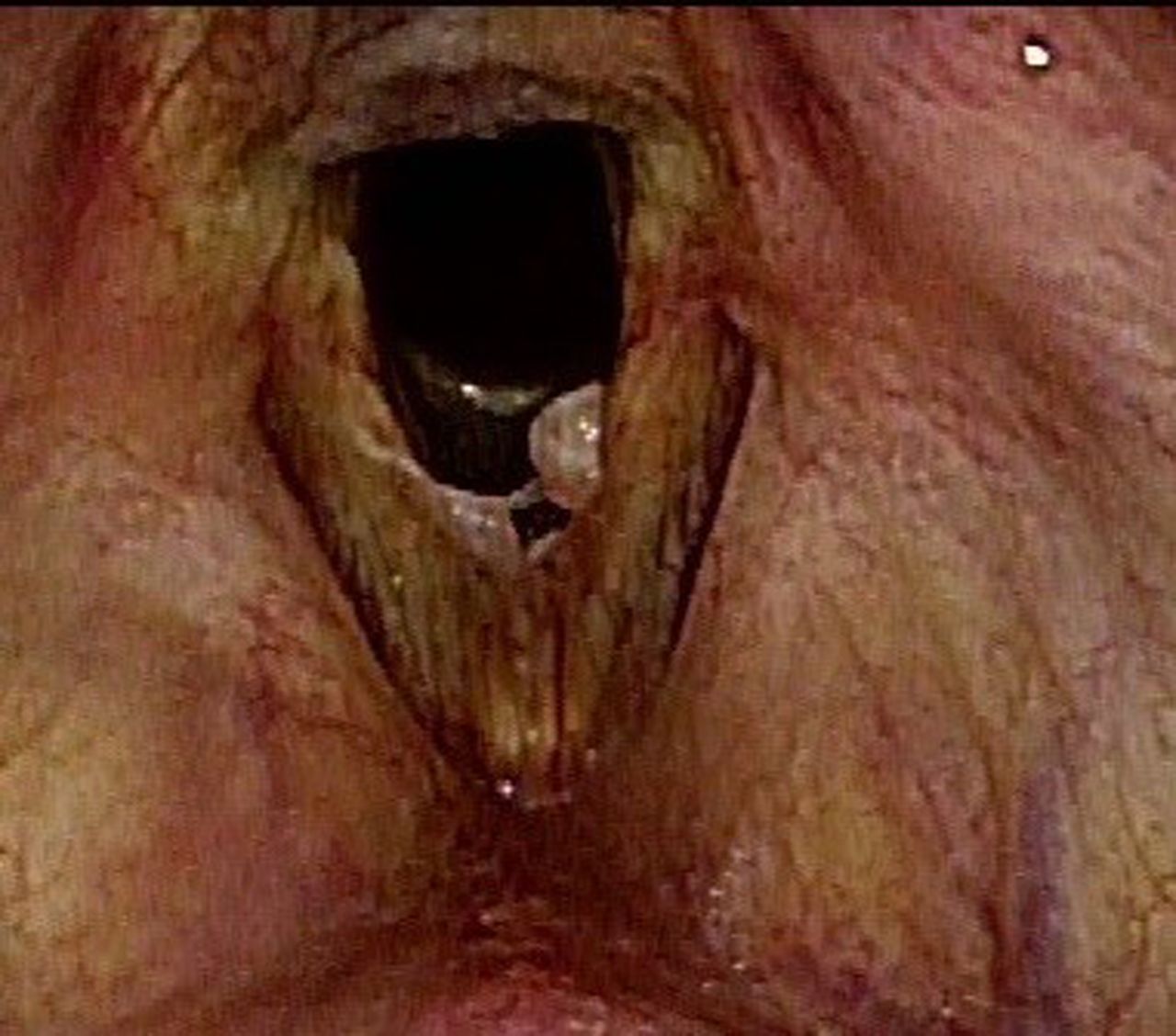
At the first examination, the laryngoscopic findings revealed milky tumours on both vocal cords and a web-like membrane with adhesions including the anterior commissure.

In the histopathological findings (H&E stain), all bilateral vocal cord tumours and the tumour in the anterior glottic web could be observed as squamous cell carcinoma with granulation formations in the background and surrounding invasion.
Outcome and follow-up
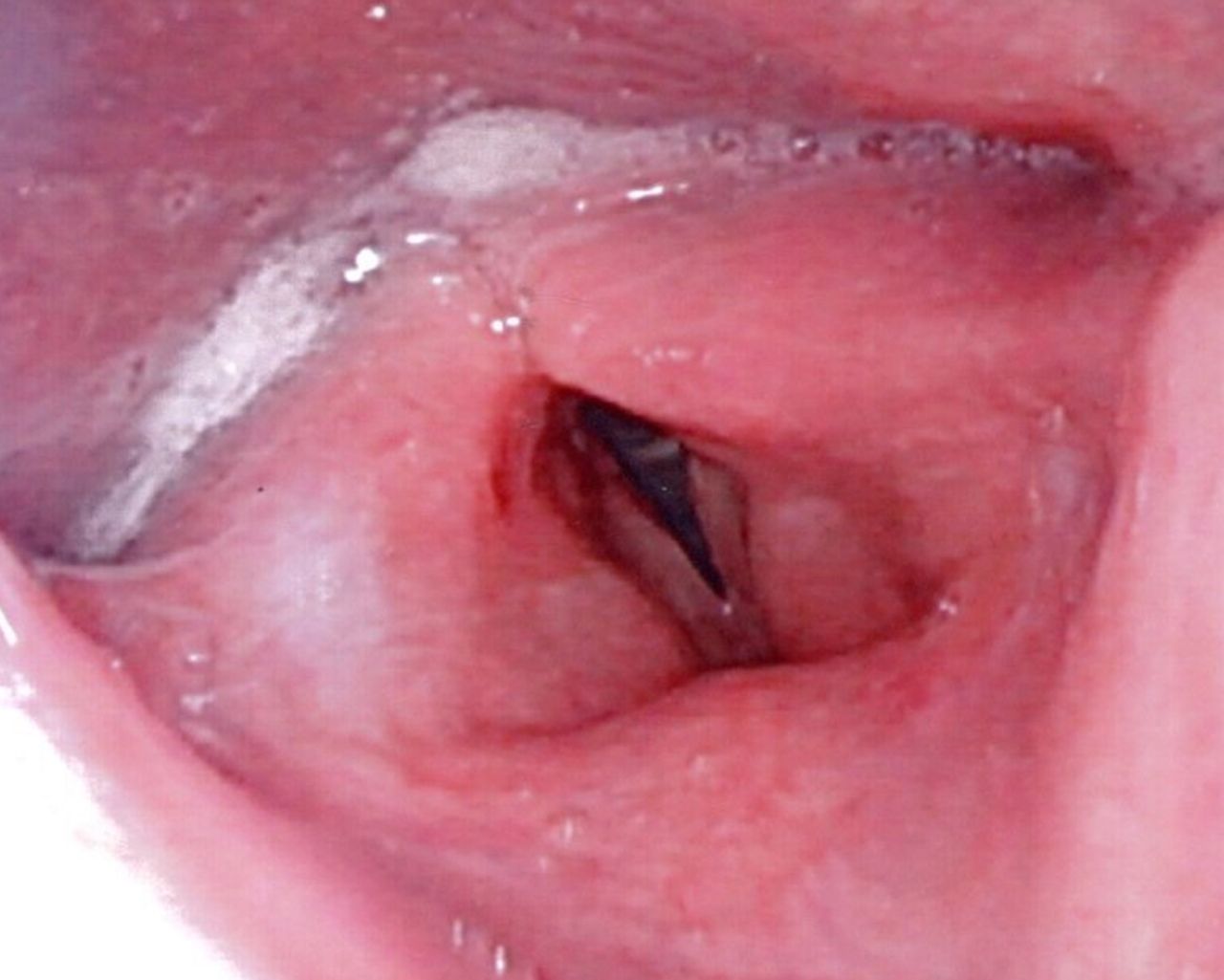
At present, he has had no recurrence of glottic carcinomas and no readhesion in the regions where the web was removed one and a half years since the end of radiotherapy (figure 3).
{kind=link}
{kind=link}
{kind=link}
The bilateral glottic carcinoma (laryngeal carcinoma (TNM classification: pT1bN0M0) with an anterior glottic web was treated with radiation therapy (66 Gy), and there has been no recurrence of the glottic carcinomas and no readhesion in the region where the web was removed one and a half years since the end of radiotherapy. The airway has remained patent.
We performed the GRBAS scale, maximal phonation time (MPT) and voice handicap index (VHI)−10 with voice evaluation before and one and a half years after the treatment. The GRBAS scale is widely performed for the evaluation of hoarseness. There are five graded scales: hoarseness (G), rough (R), breathy (B), asthenic (A) and strained (S). A four-point grading of the severity of GRBAS includes ‘0’ normal, ‘1’ slight, ‘2’ moderate and ‘3’ extreme. The GRBAS scale, MPT and VHI-10 of the pretreatment were G3R3B1A0S3, 10 s and 26. GRBAS scale, MPTand VHI-10 of post-treatment were G0R0B0A0S0, 25 s and 0. From the above findings, his hoarseness had remarkably improved one and a half years after the treatment.
Discussion
Xu et al8 mentioned that stenosis of the glottis could influence both phonation and respiration. Matrka9 recommended surgery of the anterior glottic webs for air restriction or symptomatic dysphonia. The chief complaint of our patient was hoarseness, and Hirano et al10 reported that the vocal process divides the glottis into two parts. The area of the anterior glottis is from the anterior commissure to the vocal process. The area of the posterior glottis is from the vocal process to the posterior wall of the larynx. The function and histology of the anterior glottis are phonation and stratified squamous epithelium. The function and histology of the posterior glottis are to maintain the airway and pseudostratified epithelium as one type of respiratory epithelium. Therefore, the pathophysiological differences depend on the location of the glottic adhesions. Our case was anterior glottis web and the chief complaint was hoarseness. The main symptom of the posterior glottis web would be a respiratory problem.
Sato et al11 described that anterior glottic webs are two types. One type is a laryngeal diaphragm which shows a web-like formation with adhesions including the anterior commissure. The other type is a bridge-like adhesion in the anterior glottis. Our case would correspond to the former laryngeal diaphragm type. The tissues of the glottic web showed inflammation with granulation and fibrotic scars, regardless of the causes.7 Our histopathological findings revealed the anterior glottic web with squamous cell carcinoma and granulation formations in the background. The mechanism would be considered continuous inflammation of the vocal cord cancer resulting in the formation of granulation and scarring. Cases with readhesion of the anterior glottis after operation have been reported. Hirayama et al5 performed laryngomicrosurgery in 6 cases with anterior glottic web and 4 cases experienced readhesion of the anterior glottic postoperatively. In order to prevent readhesion after cutting the anterior glottic web, Figi7 and Adachi12 suggested skin graft and fibrin coating for the wound after cutting the web. Umeno et al13 Chen14 Paniello15 and Edwards16 tried using a silicone tube and stent or keel placement. Xu et al8 described mucosal suturing of the vocal fold with placement of a stent. However, most reports including those above that were concerned with protective methods for postoperative readhesion in the anterior glottis web did not discuss the success or recurrence after a long-term follow-up. Veen17 reviewed mitomycin C in the aerodigestive tract in human studies and the follow-up period in 27 of 32 references was within 2 years or not reported. Our case was cancers of bilateral vocal cords with an anterior glottic web. Postoperative radiation therapy was administered without protective methods to prevent postoperative readhesion. After radiation therapy, we did not add it, because such methods would prevent us from determining whether there was a recurrence of anterior glottic web and glottic cancers.
Some hospitals18 19 have reported the results of CO2 laser cordectomy for gottic cancer. However, CO2 laser therapy for wide lesions with bilateral vocal cords including web would worsen the dysphonia and increase the possibility of readhesion of the postoperative wounds. Therefore, we did not select CO2 laser. Our patient underwent laryngomicrosurgery to remove laryngeal cancer tumours, and to cut-off and remove the anterior glottic web.
This simple resection and the postoperative radiotherapy showed no recurrence of the glottic carcinomas and no readhesion of anterior glottis. The reason would be considered the complete disappearance of residual cancer in the bilateral vocal cords and web by radiotherapy and re-epithelialisation of the wounds. Histopathological examination revealed the diagnosis as laryngeal carcinoma T1bN0M0. For early stage laryngeal carcinoma, radiotherapy is recommended.20–23 Moreover, since the histopathological findings in our case showed surrounding infiltration of the cancer, we considered the possibility of residual laryngeal cancer. Therefore, we administered radiation therapy (66 Gy) postoperatively. In Japan, Harada et al20 retrospectively studied the 5-year local control rates of radiotherapy for early glottic cancer (T1-T2N0) and revealed 92% in T1a, 83% in T1b (as in our case) and 86% in T2. In other countries, Zouhair et al22 described that the 5-year overall, cancer-specific and disease-free survival after radiation therapy alone in the early-stage were 80%, 94% and 70%, respectively. Jones et al23 discussed that radiotherapy and surgery for early laryngeal cancer (T1-T2 N0) were matched. The methods of the surgery included horizontal or vertical partial laryngectomy and cordectomy. The 5-year tumour-specific survival after radiotherapy and surgery were 87% and 77%. He concluded that both radiotherapy and surgery were equally effective for early laryngeal cancer. Speech and voice of the patients treated by radiotherapy were significantly better than those treated by surgery. At present, our patient has no recurrence of glottic carcinomas and no readhesion in the web region one and a half years since the end of radiotherapy. His hoarseness has completely improved. We need to continue follow-up for at least 5 years to determine whether readhesion anterior glottic web or glottic cancer has recurred.
Learning points
We encountered a case of anterior glottic web with bilateral vocal cord cancer. Commonly, histopathology of the glottic web is known to be formed from inflammation with granulations and fibrotic scarring. However, there have been rare cases, as in our case, that showed anterior glottic web with vocal cord cancer. Therefore, such cases require histopathological study using laryngomicrosurgery.
Our patient underwent radiation therapy (66 Gy) postoperatively and there has been no recurrence of the glottic carcinomas and no readhesion of anterior glottis. Some studies have presented cases in which there was readhesion of the anterior glottis postoperatively. Therefore, we should continue to follow-up.
It has reported that both radiotherapy and surgery were equally effective for early laryngeal cancer. Speech and voice of the patients treated by radiotherapy were significantly better than those treated by surgery.
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank Mr Brent Bell for reading the manuscript.
References
Footnotes
Correction notice This article has been corrected since it was online published. The funding statement has been included.
Contributors TK: diagnosis and therapy, composition of this manuscript. RW: pathological diagnosis.
Funding This work was supported in part by a Grant-in-Aid for Special Research in Subsidies for ordinary expenses of private schools from The Promotion and Mutual Aid Corporation for Private Schools of Japan.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.