Article Text

Abstract
Two patients with a laparoscopic resection of the sigmoid colon in their surgical history were diagnosed with an internal hernia because of a mesenteric gap underneath the descending neocolon. While the first case demonstrated a strongly symptomatic patient with a closed-loop obstruction of the small bowel, the second case was less obvious and correct diagnosis was achieved after a few weeks by finally performing a diagnostic laparoscopy. Since internal hernias after laparoscopic sigmoid resection are a rare complication and as presented in the second case can display very unspecific symptoms, the surgeon’s awareness is not immediately raised towards it. Therefore, an asymptomatic internal hernia bears a constant risk of a life-threatening outcome allowing to recommend an initial closure of the mesenteric gap. In both cases, successful treatment was achieved by surgery and intraoperatively closing the remaining mesenteric gap. Subsequently recovery and follow-up were uneventful.
- Gastrointestinal surgery
- General surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Colonic diverticulitis is a gastrointestinal disease characterised by inflammation of abnormal pouches—diverticula—which can develop within the wall of the large intestine. The disease is common in western countries.1
Due to a successful medical treatment of complicated diverticulitis, the indication for a surgical intervention is reserved for complicative situations including diverticular perforation, recurrent paracolic abscess formation or chronic symptomatic diverticulitis.2 3
If a patient qualifies for surgical treatment of diverticulitis, a laparoscopic approach is generally preferred due to lower perioperative morbidity and faster postoperative recovery.4
Nowadays, the technique of laparoscopic sigmoid resection is well established and represents the gold standard. To achieve a tension-free descendorectostomy, extensive mobilisation of the splenic flexure and transposition of the descending colon into the small pelvis are necessary. Complications after laparoscopic sigmoid resection include anastomotic leakage (2.9%–15.3%),5 bleeding (0.5%–1%),6 ureteral injury (1%),7 and surgical site infections (5%).8 Surgeon’s awareness of these complications needs to be high and, therefore, immediate steps for diagnosis and therapy are usually initiated.
However, other complications such as an internal hernia do occur less frequently and thus can be easily overseen due to the low specificity of symptoms.9
We herein present two cases of patients with internal hernia following laparoscopic sigmoid resection demonstrating the large variety of clinical findings and emphasising the need to consider this rare differential diagnosis in patients with abdominal pain postoperatively.
Case presentation
Case presentation 1
A female patient in her 80s presented at the emergency department with acute epigastric pain and nausea without vomiting for 4 hours. An association with eating or drinking was not observed. The patient’s further medical history showed that similar problems had occurred several times in the last weeks and months. However, these had only lasted for a few minutes. The patient’s surgical history solely indicated a previous laparoscopic resection of the sigmoid due to diverticulitis disease 9 years ago. The last defecation was reported on the previous day without any traces of blood and with normal consistency. Physical examination demonstrated a painful palpation of the upper abdomen with a slightly distended, but soft abdomen. No metallic or high-pitched bowel sounds could be heard. Blood results were normal despite a mild leucocytosis (11 g/L).
A CT of the abdomen was performed and showed a closed-loop obstruction of the small bowel (figure 1).

CT image of the abdomen: arrows point towards the closed loop (small bowel).
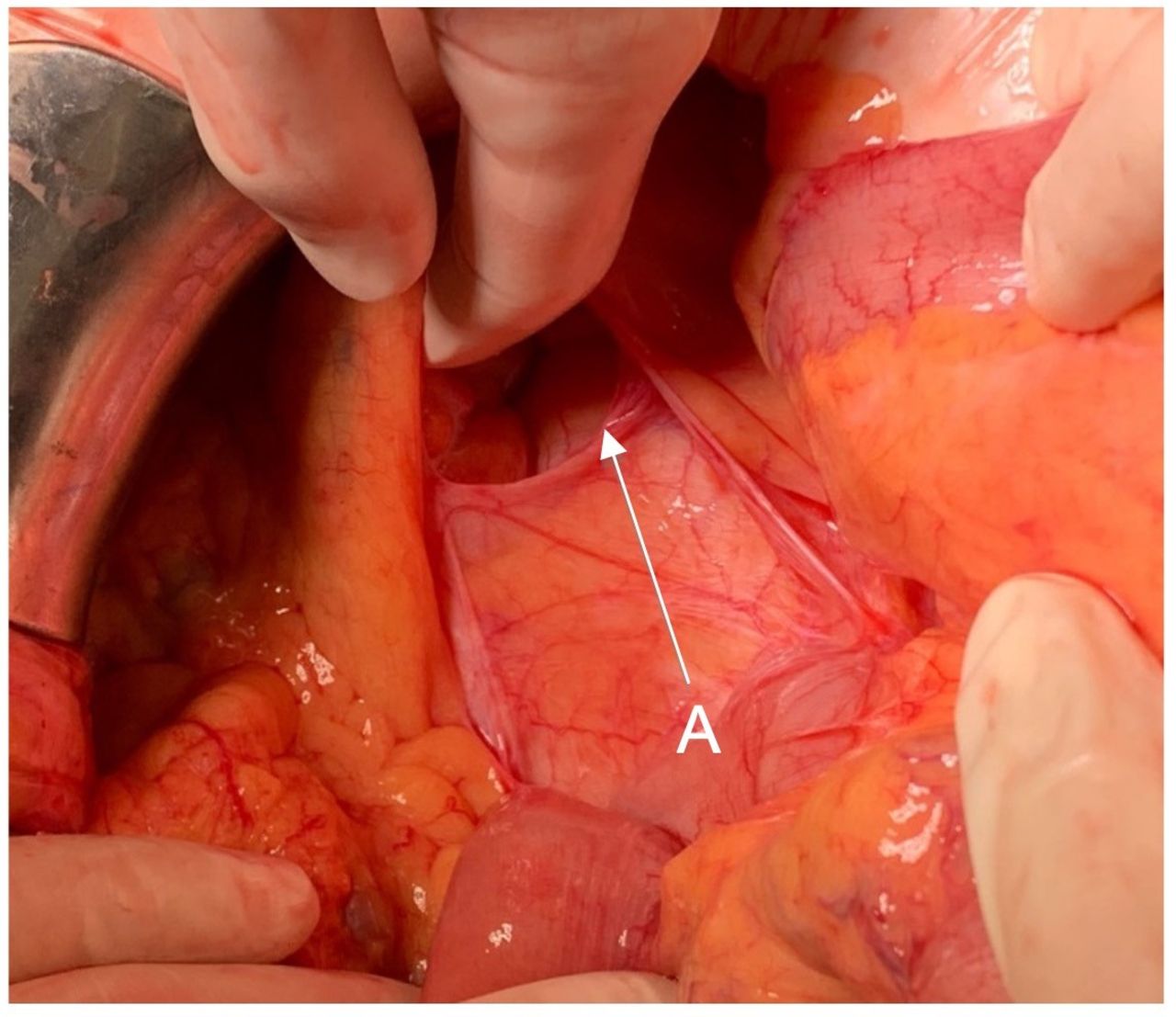
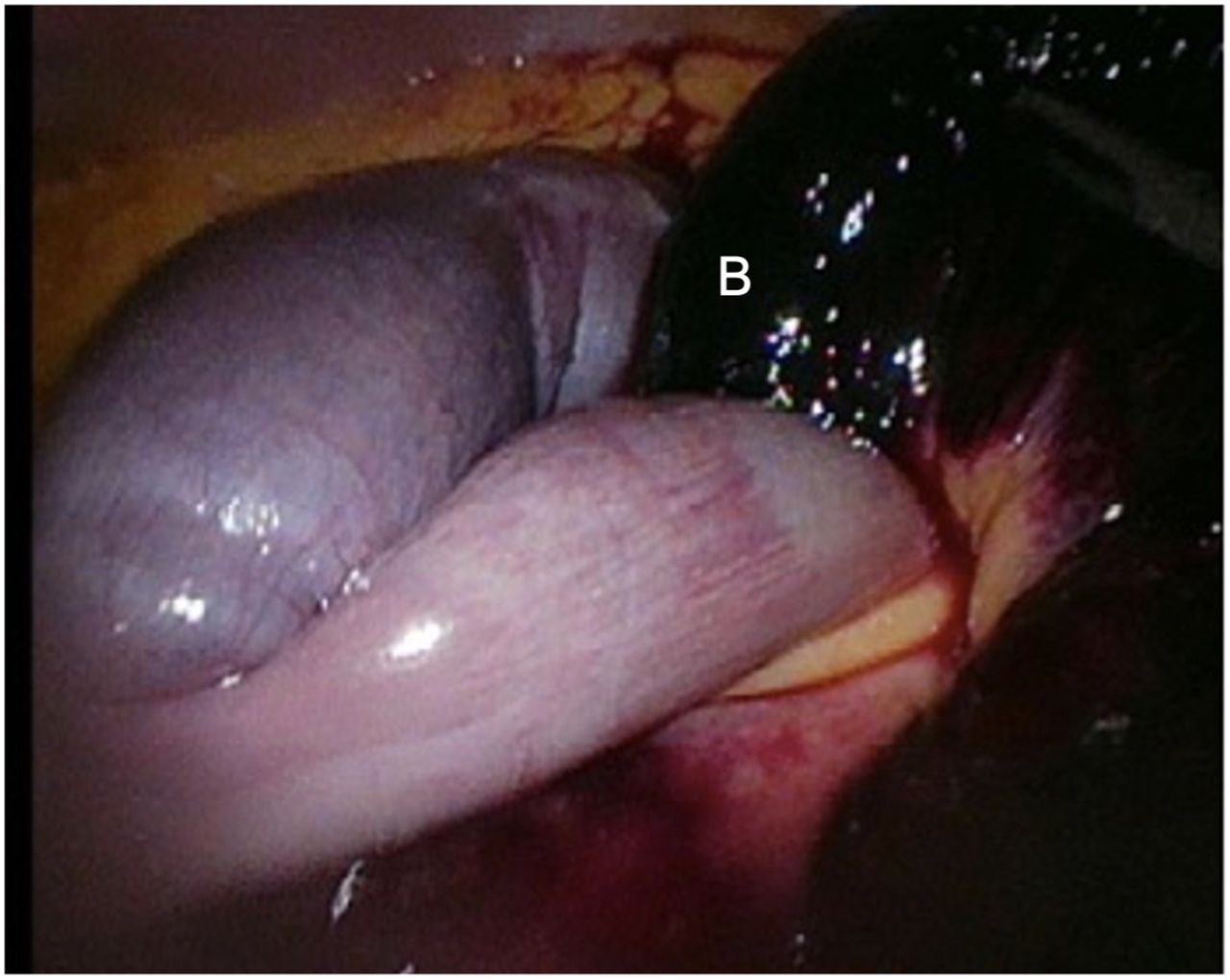
The subsequent emergency laparoscopy demonstrated an internal hernia with a jejunal loop obstructed in a residual mesenteric gap (figure 2) with signs of fatal ischaemia (figure 3). The resection of the necrotic jejunal loop with subsequent end-to-end anastomosis was performed after laparotomy. Subsequently the residual mesenteric gap was closed by a running suture with a non-resorbable thread (Ethibond 2–0).
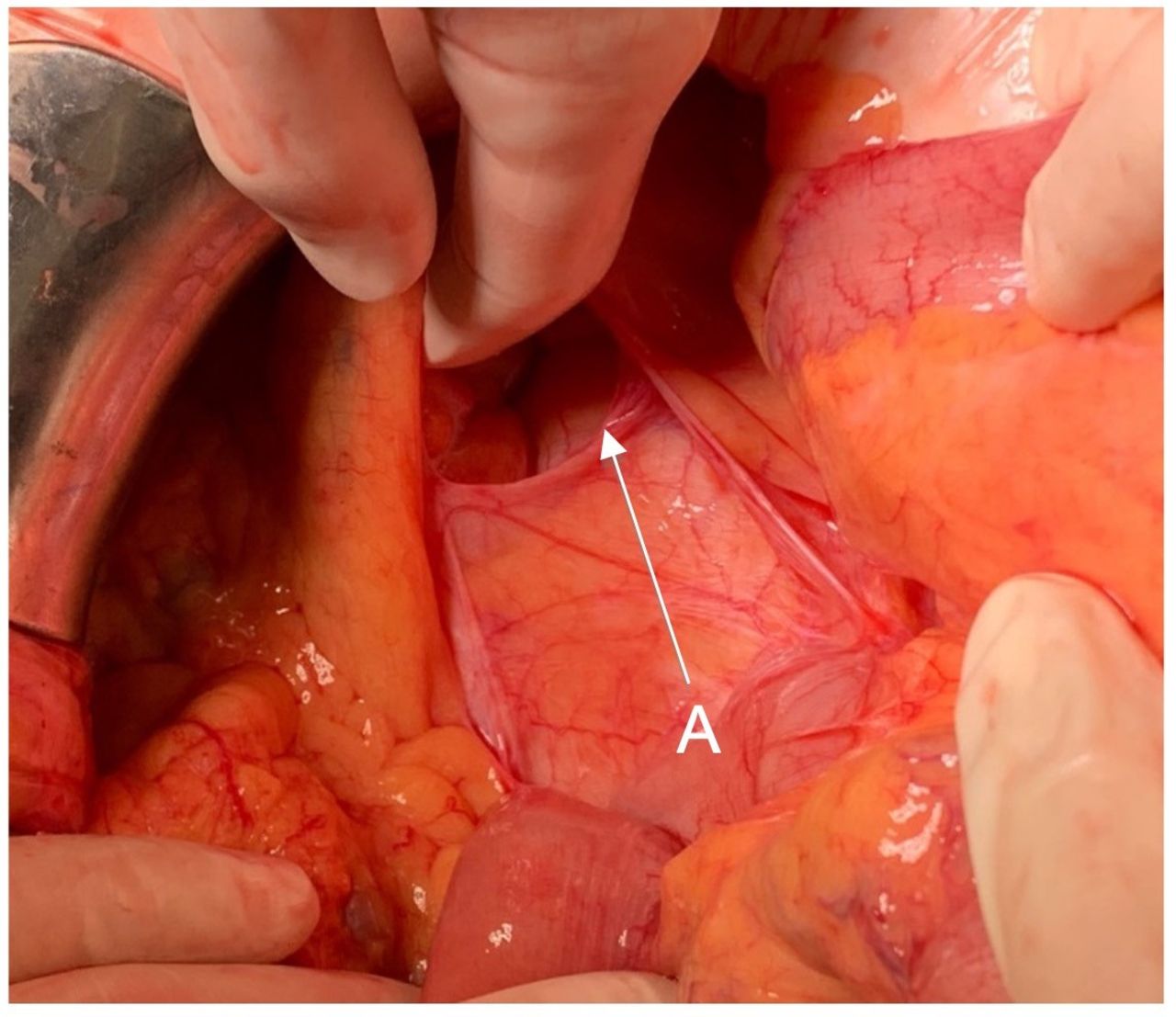
Intraoperative image of the mesenteric gap (A) after laparoscopic sigmoid resection.

Closed-loop obstruction of the small bowel with ischaemic jejunal loop (B).
Postoperative recovery was uneventful, and the patient was discharged 9 days after surgery.
Case presentation 2
A female patient in her late 70s presented with recurring abdominal pain during a period of 3 weeks. According to the patient, the pain was located predominantly in the lower abdomen, and she did not observe any association with eating or drinking. There was no nausea and emesis. Her medical history indicated a laparoscopic sigmoid resection 4 years ago due to diverticulitis disease. Furthermore, appendectomy and hysterectomy were performed more than 10 years ago. Physical examination did not indicate any pathological findings; blood results were normal.
Diagnostics via colonoscopy and CT abdomen also did not reveal the origin of complaints. The patient observed irregular bowel movement and therefore constipation was assumed which was treated medically without improvement of her complaints.
Since symptoms did not improve under conservative therapy, diagnostic laparoscopy was performed revealing a large mesenteric gap (figure 4) through which small bowel loops had migrated underneath the descending neocolon to the left side of the abdomen. The intestines were slightly distended, but without signs of acute obstruction. Position of the small bowel was corrected towards the right side and closure of the mesenteric gap was performed from Treitz ligament towards the retroperitoneum on the left side downward to the iliac vessels with a running and non-resorbable suture (Ethibond 2–0).

Laparoscopic view at the mesenteric gap (C) underneath the neocolon descendens (D).
Outcome and follow-up
Both patients had an uneventful recovery and were discharged 9 and 8 days after surgery.
Follow-up was administered after 6–8 weeks and displayed a satisfactory outcome without any signs of abdominal discomfort.
Discussion
In these two case reports, we describe the rare complication of an internal hernia with small bowel obstruction and chronic subacute abdominal pain, respectively, following laparoscopic resection of the sigmoid colon without primary closure of the mesenteric defect.
Laparoscopic resection of the sigmoid colon in diverticulitis is a very common and often performed surgery. The laparoscopic approach is generally preferred due to lower operative trauma which is associated with a decreased incidence of significant adhesions, less postoperative pain, early discharge from hospital and lower morbidity rate than open surgery.10–12
Nevertheless, it remains a surgical intervention with potential complications such as wound infection, anastomotic leakage, bleeding, ureteral injury, intraabdominal adhesions and internal hernia, with the latter being a rare complication.13
A retrospective data analysis of almost 1300 patients following laparoscopic left-sided colonic resection demonstrates a prevalence of internal hernia with small bowel obstruction and closed loop syndrome of 0.38%.14 The time between preceding surgery and clinical presentation was 0.3–10 months and thus significantly shorter than in our cases.
This finding was confirmed by another analysis of almost 200 patients following left-sided laparoscopic colonic resection reporting a prevalence of 0.5% of acute onset internal hernia requiring subsequent emergency surgery. However, this analysis also described a prevalence of 21% of asymptomatic internal hernias as confirmed by CT within 1 year postoperatively.15
There are only a few reported cases and reviews of internal hernia following laparoscopic resection of the sigmoid colon in diverticulitis. However, they all demonstrate that clinical presentation can range from asymptomatic to acute with severe bowel obstruction and subsequent ischaemia.16
The non-specificity and varying intensity of symptoms of internal hernias after laparoscopic sigmoid resection allow comparison with other surgeries in which internal hernias may also occur. Our group itself has described the problem of internal hernia after laparoscopic inguinal hernia surgery.17 Also the presence of internal hernia after laparoscopic Roux-Y gastric bypass for morbid obesity is a well-known and diagnostically challenging complication since symptoms can vary widely too.18
As demonstrated in the second case, a conclusive diagnosis can often only be made by diagnostic laparoscopy. Since minor laparoscopic surgery nowadays poses a low operative risk,19 an early diagnostic laparoscopy is advisable in unclear cases and has been implemented in our surgical department ever since.
Considering a possible life-threatening situation with incarcerated internal hernia, primary closure of the mesenteric gap between the neocolon descendens and retroperitoneum (figure 5) appears to be reasonable. If a pre-emptive closure of such a mesenteric gap can significantly reduce the incidence of internal hernia after a laparoscopic sigmoid resection can only be clarified by a controlled, randomised study in the future.
In the context of gastric bypass, these data exist and recommend the consistent closure of the mesenteric gaps.18

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Illustration (by L. Plath) of sigmoid resection (1), descending neocolon (2) with mesenteric gap and closure of mesenteric gap by suture (3).
In summary, we describe two cases of the rare complication of internal hernia after laparoscopic sigmoid resection and considering that a potentially complication-prone internal hernia occurs more frequently than assumed, we recommend primary closure of the mesenteric gap.
Learning points
Laparoscopic resection of the sigmoid colon in diverticulitis is a very common and often performed surgery. While certain complications such as anastomotic leakage are well known internal hernias are rare and therefore an awareness should be raised.
These two cases show that symptoms of internal hernias can display a wide range and particularly cases with mild symptoms can dangerously prolong the time until correct therapy is initiated.
An early diagnostic laparoscopy is advisable in cases with unspecific abdominal symptoms after laparoscopic sigmoid resection.
Asymptomatic hernias present a constant risk of a possible life-threatening outcome, allowing to recommend a primary closure of the mesenteric gap.
Ethics statements
Patient consent for publication
Footnotes
Contributors Supervised by PD Dr med AT. Patients were under care of Dr med RB, LP and PD Dr med AT. CT scans were provided and advised by Dr med CL, Department of Radiology, Spital Maennedorf. Report was written by all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.