Article Text

Statistics from Altmetric.com
Description
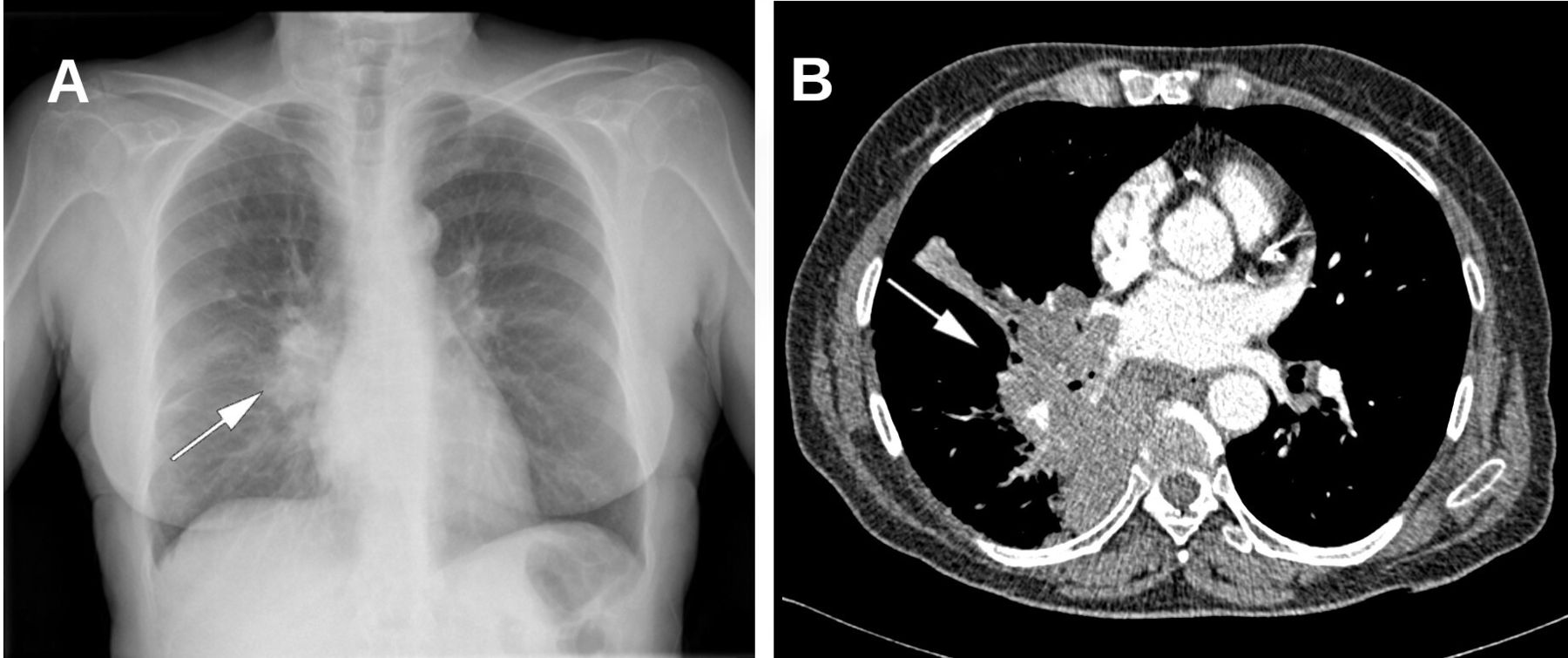
A 64-year-old female smoker was admitted to our hospital with increasing pain in the right shoulder for the prior 4–6 weeks. She also presented with a dry, non-productive cough. She denied any further symptoms, and she had no fever, weight loss or fatigue. Because of the cough, she had visited her general practitioner, who asked for a chest X-ray, which revealed a large mass in the lower lobe of the right lung, probably with right lymphadenopathies (figure 1A). The results of laboratory blood tests were normal, including white and red blood cell counts, as well as liver, lipid and kidney panels. Her primary care physician referred her to our hospital.

(A) A right pulmonary hilar tumour mass in a plain X-ray. (B) Thoracic CT scan showing a large mass with mediastinal and hilar lymph node enlargements.
Physical examination revealed no diplopia, anisocoria or ptosis but we identified a painless, solitary scalp lump (3–4 cm in diameter) that had remained unnoticed by the patient. It was not noticed by her relatives either.
Thoracic CT scan revealed a large mass in the right lobe, with multiple bilateral, mediastinal and hilar lymph node enlargements and right pulmonary vein thrombosis (figure 1B). A cranial CT scan was performed to characterise the scalp lump. It showed a solitary osteolytic lesion on the right parietal bone (4.5 cm), with bony erosion, suggesting aggressiveness; it was considered a metastasis of an unknown primary tumour (figure 2). Figure 3 shows slides of a positron emission tomography-CT scan. It showed abnormalities in the right lobe and multiple bilateral, mediastinal and hilar lymph malignant nodes with a maximum standardised uptake value of 14.87 (levels higher than 2.5 can be considered abnormal).

(A,B) A lytic lesion in the parietal bone of the skull. (C,D) A 3D reconstruction.

{kind=link}
{kind=link}
{kind=link}
(A,B) Intense 18F-labelled 2-fluoro-2-deoxyglucose uptake in the right lobe and several bilateral, mediastinal and hilar lymph pathological nodes, when the patient underwent a positron emission tomography-CT scan.
The patient underwent a bronchoscopy, which revealed incomplete obstruction of the right main bronchus and complete obstruction of the right middle lobe bronchus. A biopsy was obtained, which revealed non-small-cell lung cancer. Immunochemistry staining was positive for thyroid transcription factor-1 and negative for p63, which confirmed the histopathological diagnosis.
Further investigation revealed bone and liver involvement (metastases to parietal bone, thoracic and lumbar vertebrae and scapular bone). The patient underwent chemotherapy treatment with carboplatin–pemetrexed. The patient was also referred to radiotherapy oncologists for radiotherapeutic treatment (five cycles of 400 cGy), but it was suspended because her clinical condition rapidly worsened. The patient passed away 4 months after the diagnosis.
It is worth noting that echinoderm microtubule-associated protein-like 4 (EML4)-anaplastic lymphoma kinase (ALK)-positive lung cancer is associated with lung adenocarcinoma, the main differential diagnosis proposed by our pathologist. Likewise, epidermal growth factor receptor (EGFR)-positive cells are associated with non-small-cell lung cancer. Unfortunately, these immunochemistry techniques were not available at our pathology laboratory at the time of the diagnosis of our patient (2016). This is an interesting aspect of the case because our patient underwent a carboplatin–pemetrexed regime, instead of taking EML4-ALK-positive or EGFR-positive lung-tumor-specific drugs, such as crizotinib, ceritinib, afatinib or erlotinib.
Primary tumours of the skull are uncommon, but up to 80% of secondary bone scalp tumours are malignant1 and their differential diagnosis can be broad (cysts, fibrous dysplasia, osteomyelitis, etc). Regarding metastases, the most frequent are breast, lung and prostate.2 Moreover, skeletal metastases in lung cancer can be present in up to 36% of patients, with the spinal cord being the most common location.3 This emphasises that lung cancer is often diagnosed in an advanced stage. Skull metastases, however, are uncommon even in advanced stages of tumours, although some cases have reported of temporal,4 5 calvarian6 7 or frontal8 metastases as the initial manifestation of lung cancer. These metastases are usually lytic and pain is the main manifestation, which decreases patients’ quality of life. That is why therapy is often focused on reducing the pain and improving functionality, but this management is often palliative, not curative. Pain, neurological involvement and instability of lesions are the main indications for radiotherapy, as was the case for our patient.
Learning points
Malignant lung tumours may be diagnosed at advanced stages, due to minimal symptoms of the disease.
Spinal cord and axial metastases are common in the natural history of some types of cancer, such as lung tumours.
Pain and the improvement in functionality and in quality of life are the main goals of therapy for lung cancer in an advanced stage with metastatic disease, that is, the treatment is for palliative rather than curative purposes. Notwithstanding, clinicians should be aware of the poor prognosis of these patients.
Ethics statements
Patient consent for publication
Footnotes
Twitter @my_phd_life
Contributors RGC wrote the first draft. MO-G and SH-P reviewed the manuscript and provided important contributions. PA-B was the radiologist who rendered the skull images in 3D.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.