Article Text

Statistics from Altmetric.com
Description
A man in his late 40s presented with complaints of non-radiating, dull aching chest pain that were non-aggravating on exertion and associated with palpitations. He had no history of fever, dyspnoea, weight loss, pedal oedema, night sweat or loss of appetite. No history of similar complaints in the past. Family history was negative. Vital signs were within normal limits: respiratory rate of 19 breaths per minute, heart rate of 102 beats per minute, blood pressure of 118/76 mm Hg, oxygen saturation of 92% at room air and temperature of 98.6 degrees Fahrenheit. On auscultation, breath sounds were normal. Routine laboratory investigations performed were within normal limits (RBC 3.6×1011/L, haemoglobin 120 g/L, WBC 7.8×108/L, platelet count of 200×109/L, haematocrit 37 vol%, troponin I <30 ng/L and random blood glucose 110 mg%). The spirometric test showed the normal forced expiratory volume (FEV) of 2.66, normal forced vital capacity (FVC) of 3.34, normal forced expiratory flow of 3.58, normal FEV/FVC of 79.71 and normal peak expiratory flow rate of 8.57.
Chest radiograph (figure 1A,B) demonstrated reduced right lung volume, absent right hilar shadow, with hemidiaphragm elevation, ipsilateral mediastinal shift and hyperinflation of contralateral lung. CT scan of chest performed followed by CT pulmonary angiography (figure 2A–F) demonstrated absent right pulmonary artery, with numerous collaterals from an engorged tortuous bronchial artery, posterior intercostal arteries arising from descending thoracic aorta and branches from engorged subclavian artery. Reduced right lung volume and mediastinal shift towards right were noted. The main pulmonary artery appeared dilated (approximately 30 mm) suggestive of pulmonary hypertension.

Chest radiograph (A) and schematic diagram (B) demonstrating reduced right lung volume with shift of mediastinum to right and absent right hilar shadow with compensatory hyperinflation of left lung. Note the normal left hilum (black arrow).
{kind=link}
{kind=link}
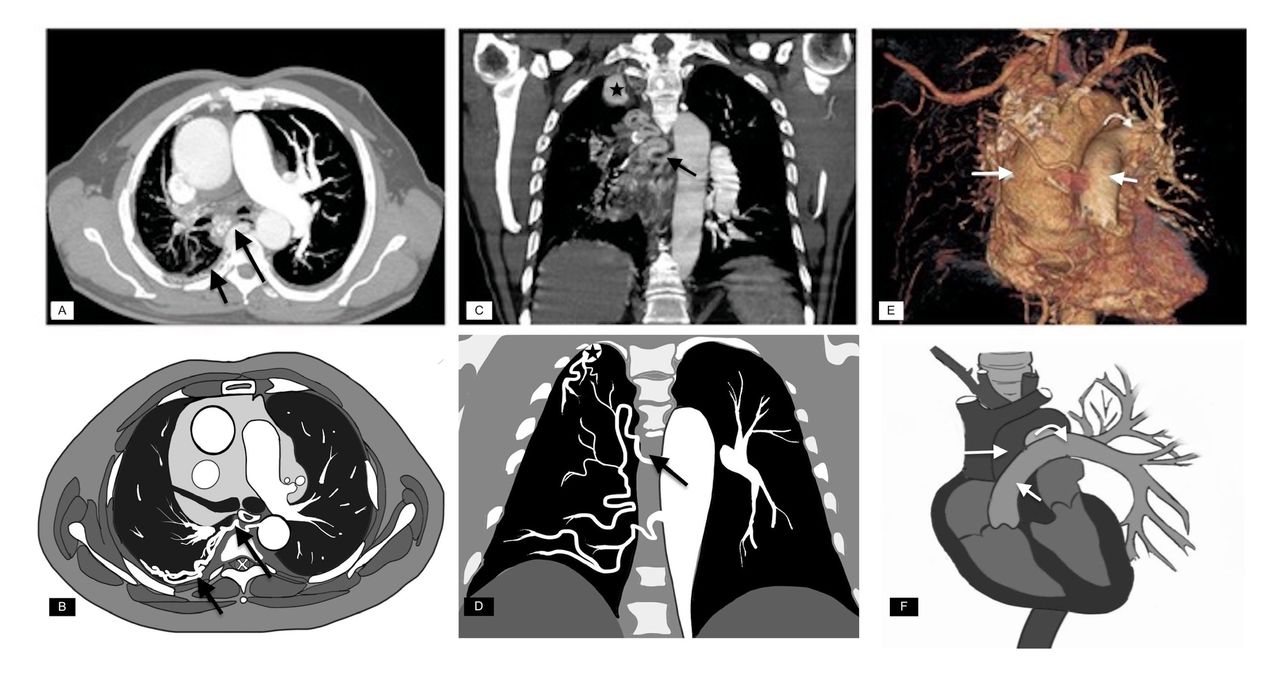
Axial maximum intensity projection image (A) and schematic diagram (B) of the chest at pulmonary artery level demonstrating absent right pulmonary artery with reduced right lung volume and mediastinal shift to right. Note the absence of right hilar vessels and presence of prominent tortuous collateral circulation from right posterior intercostal arteries (short arrow) and right bronchial artery (long arrow). Coronal maximum intensity projection image (C) and schematic diagram (D) of pulmonary angiogram demonstrating prominent tortuous right bronchial artery (black arrow) and prominent right subclavian artery (asterisk). 3D volume rendered (surface-shaded display)-computed tomographic image (E) and schematic diagram (F) demonstrating absent right pulmonary artery with extensive collaterals in right hemithorax. Note arch of aorta (long white arrow), main pulmonary artery (short white arrow) and left pulmonary artery with hilar vessels (curved arrow).
The radiological features were consistent with the absence of the right pulmonary artery. The patient is treated for pulmonary hypertension with tablet warfarin 5 mg and tablet bosentan (an endothelin receptor antagonist) 32 mg and advised for follow-up. On follow-up, after 1 month significant improvement in the clinical symptoms was noted.
Unilateral agenesis of pulmonary artery is a rare condition with prevalence of about 1:200 000.1 Embryologically, agenesis of the pulmonary artery is due to failure of migration and rotation of primitive sixth aortic arch. Right-sided agenesis is usually not associated with cardiac anomalies, hence may be termed as isolated unilateral agenesis of the pulmonary artery (UAPA). Left-sided agenesis is often associated with cardiac abnormalities (hence non-isolated), thus early diagnosis and surgical repair may be necessary during early childhood. Infants with isolated pulmonary artery agenesis may present either with respiratory distress, pulmonary hypertension and congestive cardiac failure or remain asymptomatic until adulthood which may delay the diagnosis. Presentation in an adult patient can be variable with symptoms of chest pain, exertional dyspnoea, exercise intolerance, recurrent pulmonary infections, haemoptysis and pulmonary hypertension which are the most common presentations among the adult population with the mortality rate being 7%–8%.2 3 Symptoms may sometimes be provoked by pregnancy or high altitude. Complications of isolated (right) UAPA may include massive haemoptysis and extensive recurrent pulmonary infections.
Chest radiograph is the first line investigation for UAPA. Echocardiography may be helpful in diagnosis and also to assess the presence of associated pulmonary hypertension. CT and MRI are the imaging modalities for the detailed anatomical depiction of UAPA. CT angiography remains to be the gold standard and modality of choice for diagnosis of UAPA.
CT angiogram demonstrates the collaterals which arise from descending thoracic aorta by bronchial, intercostal, subdiaphragmatic branches and subclavian or coronary arteries. The affected lung is frequently perfused by the bronchial artery,.4
Treatment of isolated UAPA is usually individualised and is based on symptoms and associated conditions and is usually by medical or surgical approach. In case of intractable pulmonary infections or recurrent haemoptysis, either pneumonectomy or lobectomy is performed. In patients with massive haemoptysis, embolisation of bronchial arteries is usually the procedure of choice.5
Patient’s perceptive
After treatment, I was relieved of symptoms and was counselled about my clinical condition and advised for regular follow-up every 6 months.
Learning points
Agenesis of the pulmonary artery is a rare congenital vascular anomaly. Right-sided agenesis is isolated, hence termed as isolated unilateral agenesis of the pulmonary artery (UAPA). Left-sided agenesis is usually more frequently associated with cardiac anomalies (UAPA).
Isolated UAPA may have a delayed or asymptotic presentation and may survive into adulthood. Symptomatic patients in adults require treatment and follow-up. Few of these patients may present with massive haemoptysis and intractable pulmonary infections.
CT angiogram plays a vital role in demonstration of collateral circulation in these patients for therapeutic management.
In case of massive haemoptysis and persistent pulmonary infection, interventional embolisation of vessels or surgical management is mandatory.
Ethics statements
Patient consent for publication
Footnotes
Contributors RKN: Overall preparation and editing of the manuscript. MA: Preparation of the manuscript draft. RJ: Review of literature and references. SS: Preparation of line diagrams and technical work of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.