Article Text

Abstract
A woman in her 30s who was 12 weeks pregnant with her third child presented with jaundice. Blood tests showed elevated hepatobiliary enzymes and direct bilirubin. Abdominal ultrasonography showed dilatation of the common bile duct and strong echo with a 9 mm acoustic shadow in the distal bile duct. She was diagnosed with common bile duct stone disease and biliary drainage was considered necessary. Percutaneous transhepatic biliary drainage (PTBD) was performed considering the effect on both the fetus and the mother, and the procedure was successful without any complications. The PTBD tube was left in place until delivery at 36 weeks 6 days of gestation and endoscopic stone removal was performed 14 days after delivery. The patient was discharged 18 days after delivery without any complications. In pregnant women with common bile duct stones, palliative PTBD followed by elective endoscopic stone removal after delivery can be considered a treatment strategy.
- biliary intervention
- endoscopy
- pregnancy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
No established guidelines exist on the treatment of common bile duct stone disease with obstructive jaundice in pregnant women. Biliary drainage may be required, potentially with stone removal at a later stage, and is the safest treatment for both the mother and the child. This is usually performed by a non-surgical approach. We herein review the treatment options for this condition in the context of a recent case involving a pregnant woman with common bile duct stones who underwent palliative percutaneous transhepatic biliary drainage (PTBD) followed by elective endoscopic stone removal after delivery.
Case presentation
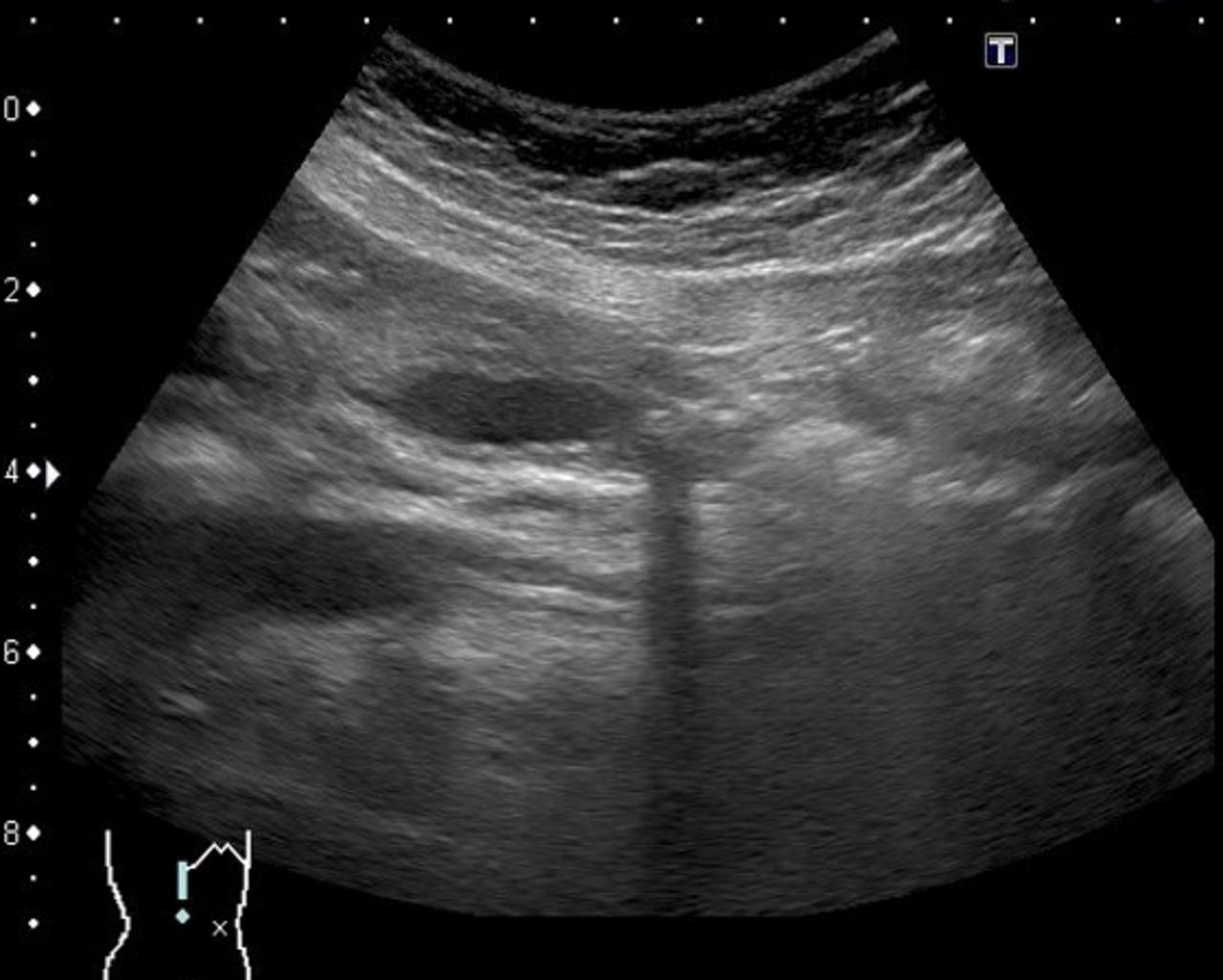
A woman in her 30s who was 7 weeks 4 days pregnant with her third child developed nausea and icterus. Blood tests showed elevated levels of hepatobiliary enzymes and direct bilirubin (table 1). Abdominal ultrasonography showed dilation of the common bile duct to 10 mm and strong echo with a 9 mm acoustic shadow in the distal bile duct (figure 1). The patient was admitted to our facility with a diagnosis of obstructive jaundice associated with common bile duct stones. However, acute cholangitis was considered to be absent because the patient had neither significant symptoms such as abdominal pain or fever nor evidence of inflammation on blood test. The patient was placed under observation because there was no sign of acute cholangitis and we were concerned about the effects of radiation exposure on the fetus in the seventh week of pregnancy, during which organogenesis takes place. Fortunately, the patient’s condition improved without biliary drainage and she was discharged. However, she developed nausea at 12 weeks 1 day of pregnancy and her blood test showed elevated hepatobiliary enzymes (table 1). She was admitted to our hospital due to recurrent obstructive jaundice associated with common bile duct stones. Although she did not have cholangitis or pancreatitis at admission, we considered that biliary drainage was required due to the short-term recurrence.
Blood test results
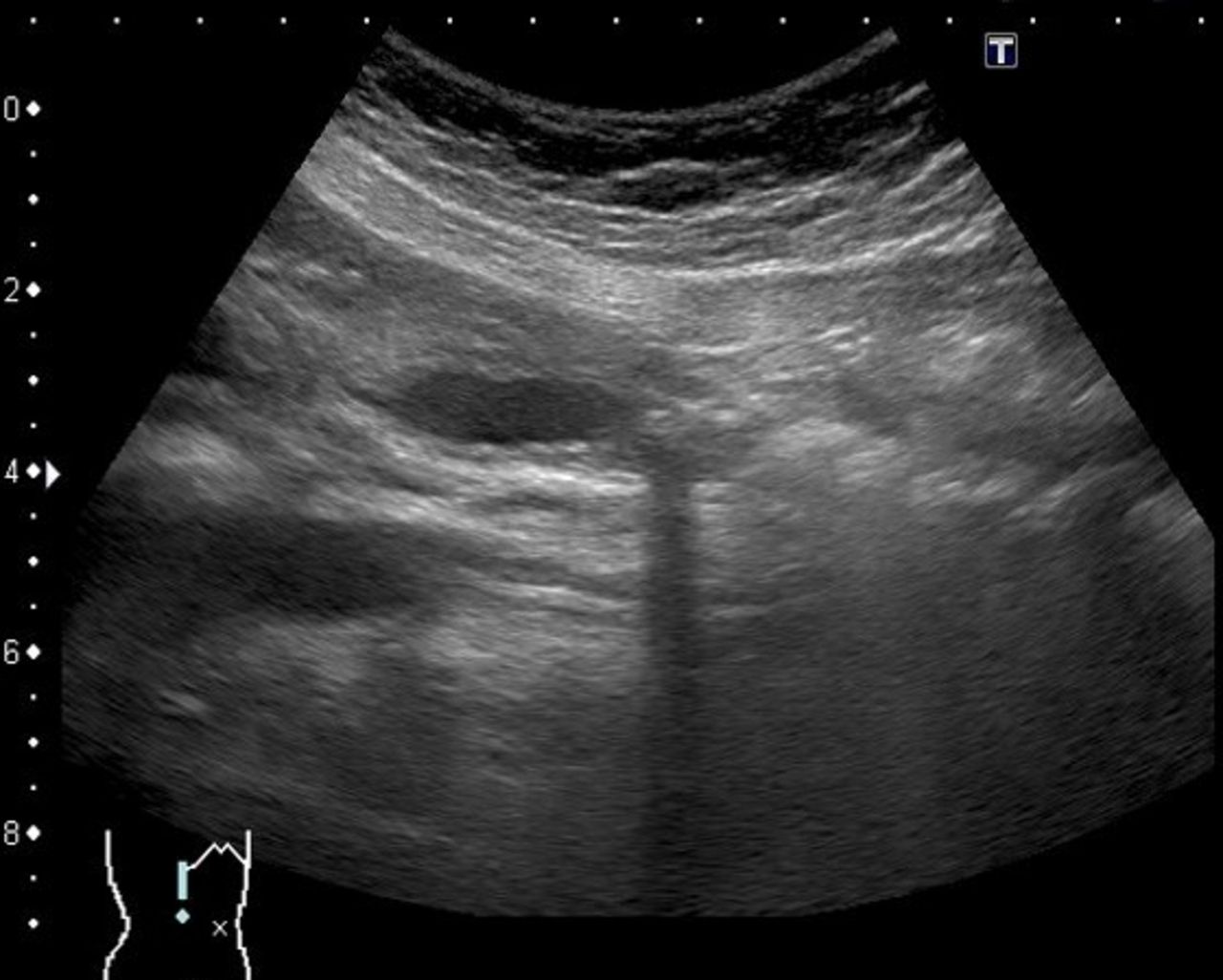
Abdominal ultrasonography revealed strong echoes in the distal bile duct with a 9 mm acoustic shadow.
Investigations
When similar symptoms again developed, the patient’s blood tests showed elevated levels of hepatobiliary enzymes and direct bilirubin. White cell count and C reactive protein level were within the reference range (table 1).
Treatment
After consulting with the obstetrician and obtaining the patient’s fully informed consent, PTBD was performed at 12 weeks 3 days of gestation. PTBD tube contrast examination revealed two defects in the distal bile duct, indicating the presence of stones of about 9 mm in diameter (figure 2). After treatment, the patient’s symptoms and jaundice improved. She was discharged 19 days after the tube was placed. With the tube in place, she gave birth at 36 weeks 6 days of pregnancy without complications. On the 14th day after delivery, endoscopic stone removal was performed by endoscopic retrograde cholangiopancreatography (ERCP) and the PTBD tube was removed to help the obstetrician and internist (figure 3).

Percutaneous transhepatic bile duct drainage tube contrast examination revealed two defects in the distal bile duct that were considered to be stones of about 9 mm.

ERCP test revealed that the stones had been removed. ERCP, endoscopic retrograde cholangiopancreatography.
Outcome and follow-up
At the time of this writing, the patient had been doing well for 4 years without any recurrence of the common bile duct stones. There were no abnormalities in the growth of the child.
Discussion
Methods of biliary drainage in patients with common bile duct stones and cholangitis include endoscopic transpapillary biliary drainage by ERCP, percutaneous biliary drainage and endoscopic ultrasonography-guided biliary drainage (EUS-BD). The treatment method should be determined with consideration of the effect on the fetus as well as the pregnant mother. Regardless of which biliary drainage method is selected, there is concern about the effects of radiation exposure on the fetus. The dose on the X-ray incident surface on normal fluoroscopy is 10–20 mGy/min. Even with only 5 min of fluoroscopy, the skin receives radiation exposure to 100 mGy. The risk associated with radiation exposure depends on the developmental period of the fetus, which is divided into the preimplantation phase (0–8 days after fertilisation), the organogenesis phase (2–15 weeks after fertilisation) and the fetal phase (15 weeks after fertilisation). Table 2 shows the risks associated with radiation exposure in each period.1 2 The fetus in the present case was in the organogenesis stage. Although it has been reported that the incidence of malformations is not high at radiation exposure doses of less than 50 mGy, radiation exposure should be avoided as much as possible because this is a period of high radiation sensitivity.3 Various reports have described cases in which ERCP was performed with consideration of radiation exposure to pregnant women. In one case, ERCP was performed without fluoroscopy, an endoscopic sphincterotomy was performed and a bile duct stent was placed, and ERCP was performed again after delivery for stone removal.4 In another case, the number of stones was identified by endoscopic ultrasonography, ERCP was performed without fluoroscopy, and the number of stones removed was confirmed.5 However, ERCP without fluoroscopy requires a skilled operator and assistant. Additionally, placement of a bile duct stent without confirming the location of the stones may make drainage less reliable. On the other hand, because percutaneous biliary drainage is a treatment performed under echo guidance, the guidewire can be visually recognised. Therefore, percutaneous biliary drainage is considered to shorten the fluoroscopy time as compared with endoscopic biliary drainage. Both ERCP and EUS-BD involve endoscopy. The first problem with endoscopy in pregnant women is the safety of sedatives or analgesics; however, these drugs are essential for safe endoscopy. The use of sedatives in pregnant women is associated with a risk of fetal hypoxia in the event of oversedation. Some sedatives have also been reported to be teratogenic and associated with a risk of preterm birth.6 7 Although benzodiazepines are commonly used for sedation in endoscopic treatment, they are category D drugs in the classification of the US Food and Drug Administration.7 Propofol (category B) is a drug that can be used relatively safely during pregnancy, but should be administered by an anaesthesiologist. Therefore, it is difficult to use propofol in settings without an anaesthesiologist, such as during emergency treatment. Furthermore, endoscopic biliary drainage is usually performed from the prone position to the left lateral position, but this position may not be possible due to pregnancy. There is a risk that the safety of treatment cannot be maintained due to difficulty in maintaining the correct posture for the procedure. One of the most important complications of ERCP is post-ERCP pancreatitis. The incidence of post-ERCP pancreatitis in therapeutic ERCP-related procedures reportedly ranges from 3.1% to 5.4%.8 Pregnancy is a reported risk factor for post-ERCP pancreatitis.8 9 Several reports have addressed the safety of ERCP in pregnant women.3 10 11 Post-ERCP pancreatitis in pregnant women has a clear relationship with both fetal complications and intrauterine fetal mortality (3.8%).12 13 Therefore, post-ERCP pancreatitis is a complication that must be avoided in pregnant women. EUS-BD requires advanced technology and has a high incidence of complications such as biliary peritonitis; therefore, it is performed only in limited facilities. In the present case, after discussing these risks with an obstetrician/gynaecologist, the patient and the patient’s family, PTBD was selected. This treatment is associated with potential complications such as bleeding, biliary peritonitis, pneumothorax and biliary infection. PTBD is not an indicated procedure in all cases because the degree of bile duct dilation is related to the success rate of the procedure; however, it can be performed in many hospitals. No reports to date have described PTBD in pregnant women, and this is the first such report. PTBD has important advantages in terms of its reduced radiation exposure compared with endoscopic biliary drainage, no sedation-related problems and no risk of post-ERCP pancreatitis. It also does not require advanced and special medical techniques, which differs from EUS-BD, and it is a generally widespread procedure. Therefore, it is possible to perform PTBD in an emergency setting. PTBD and ERCP are common biliary drainage techniques used in emergency situations. Table 3 presents a comparison between these two treatments to help clinicians choose a less invasive procedure in an emergency. The biggest disadvantage of PTBD is the need to manage the external fistula tubes. As the fetus grows, abdominal circumference increases, causing the tube position to fluctuate and the risk of tube dropout to increase. We have endeavoured to reduce the risk of external fistula problems by thoroughly educating patients in tube management and treatment. At our hospital, the tube insertion part is usually fixed with two needles; to prevent the tube from falling off, however, a third needle is added for stronger fixation. By making a hole in the inserted tube, biliary drainage is possible even when the tube tip is in the duodenum. By placing the tip of the PTBD tube into the duodenum after stabilising the fistula, we believe that we have contributed to reducing the risk of tube dislodgement. Other problems with PTBD are the length of hospital stay and pain. Hospitalisation is required at least until the fistula is stable, which will take a minimum of 1 week. A hospital stay of 2 weeks or longer may be required, along with tube education. In the present case, the patient required 19 days of hospitalisation after PTBD. For biliary drainage procedures other than PTBD, discharge from the hospital within 1 week is possible without complications. Pain can be caused by intra-abdominal leakage during insertion or can occur after the tube is inserted. Adequate local anaesthesia and intravenous analgesics are also considered as options to reduce the pain that occurs during tube insertion. Pain after tube insertion may continue until the fistula is stabilised and should be treated with rest and analgesics. The pain may cause nausea and vomiting and risk of tube dropout. An option in some cases may be tube removal after the symptoms have improved or if pain persists. Table 4 presents the advantages and disadvantages of PTBD. The risk of intra-abdominal leakage may still be lower than the risk of post-ERCP pancreatitis. To reduce the risk of intra-abdominal leakage, the procedure should be performed as smoothly as possible and managed with analgesics. It is especially important to shorten the tube insertion time after dilatation. We selected PTBD for a case of common bile duct stones with obstructive jaundice in a pregnant woman and we were able to safely perform biliary drainage without adverse events. The patient was able to continue her pregnancy without complications after insertion of the drainage tube; the drainage tube was left in place until delivery and the common bile duct stones were removed after delivery. This treatment option is considered a feasible way to treat common bile duct stones in pregnant women. Figure 4 shows a timetable for optimal treatment of similar cases. First, cholangitis should be diagnosed and its severity assessed. In cases of severe cholangitis, surgery or biliary drainage is required. Surgical treatment is performed when other treatments are difficult. For patients with mild to moderate disease or no cholangitis, conservative therapy is the treatment of choice. Generally, if the patient improves with conservative treatment, he or she will be observed and stone removal will be performed after delivery. If the patient does not improve with conservative treatment, biliary drainage should be considered. Risks of not performing biliary drainage include worsening of symptoms and the development of cholecystic pancreatitis, which may increase mother and infant mortality. Risks of performing biliary drainage include radiation exposure, adverse events and the effects of sedatives and analgesics on the fetus. Clinicians should consult with the obstetrician, anaesthesiologist, radiologist, surgeon and gastroenterologist to determine the most appropriate biliary drainage procedure. In this decision-making process, the risks associated with each drainage procedure should be considered (table 5). Based on the above, it is important to choose the most appropriate treatment and thoroughly explain the treatment plan to the patient.
Effects of radiation exposure on the fetus
PTBD versus ERCP
Advantages and disadvantages of PTBD

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Algorithm for optimal treatment of common bile duct stones in pregnant women.
Risk of biliary drainage
Learning points
Percutaneous biliary drainage can be an option for biliary drainage in pregnant women.
When a percutaneous biliary drainage tube is placed in a pregnant woman, it is possible for the patient to continue the pregnancy and give birth under the condition of external fistula management.
Percutaneous biliary drainage may well be one of the safer options for biliary drainage in pregnant women.
Ethics statements
Patient consent for publication
Acknowledgments
We gratefully acknowledge Dr Naotaka Fujita, Dr Hiroyuki Maguchi and Dr Takao Itoi for their valuable advice in this case. We also thank Angela Morben, DVM, ELS, from Edanz (https://jp.edanz.com/ac), for editing a draft of this manuscript.
Footnotes
Contributors KK: planning, conduct, reporting of the work, writing the original draft. MT, SW: planning, conduct, manuscript review and editing. TH: planning, manuscript review and editing, supervision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.