Article Text

Abstract
A woman in her mid-30s presented to the orthopaedic team, unable to mobilise, shortly after her caesarean section. On questioning, she reported 10 weeks of atraumatic right hip pain. A radiograph revealed a displaced right subcapital neck of femur fracture. An MRI confirmed this, as well as identifying a minimally displaced left subcapital neck of femur fracture. She underwent a right total hip replacement and internal fixation of the left hip. A dual energy X-ray absorptiometry (DEXA) scan showed severe osteoporosis, and a diagnosis of transient osteoporosis of the hip was made. She was seen by the bone metabolism team and given calcium and vitamin D medication. Although atraumatic hip fractures are rare in young patients, disproportionate or persisting hip pain in pregnant patients should raise the index of suspicion and prompt further investigation in the form of an MRI. This will allow timely management of hip fractures and improve patient outcomes.
- Obstetrics, gynaecology and fertility
- Calcium and bone
- Hip prosthesis implantation
- Musculoskeletal and joint disorders
- Orthopaedic and trauma surgery
Statistics from Altmetric.com
- Obstetrics, gynaecology and fertility
- Calcium and bone
- Hip prosthesis implantation
- Musculoskeletal and joint disorders
- Orthopaedic and trauma surgery
Background
Bilateral neck of femur fractures is a rare condition usually associated with high-energy trauma or poor bone quality with known metabolic disorders. Transient osteoporosis of the hip (TOH) is an uncommon condition where its prevalence, aetiology and pathogenesis are not fully understood, and its absolute risk factors remain unclear. TOH, which can predispose young women to fractures, has been mainly documented in case reports as vertebral fractures most commonly occurring in the third trimester or postpartum period.
There is currently no systematic analysis on this condition in literature. TOH is likely to be underassessed, and a low index of suspicion is required to investigate pregnant patients presenting with significant pain without adequate trauma. This will aid in the prevention and optimal management of fractures. Particularly of the hip where timely intervention can improve outcomes.
We present an extremely rare case of a woman in her mid-30s with atraumatic bilateral femoral neck fractures sustained during the third trimester of pregnancy.
Case presentation
A primigravida in her mid-30s was referred to our orthopaedic team on the day of her elective caesarean section. Her right leg had given way, and she was unable to mobilise immediately post partum. The patient described atraumatic right hip pain since week 28 of pregnancy. Initially, this was considered pregnancy-related musculoskeletal pain by the obstetricians as there was no trauma, and she was supplied with crutches and eventually required a wheelchair. She also reported to a lesser degree left hip pain of more recent onset. The patient had requested an elective caesarean section at 37 weeks+4 due to worsening pelvic pain and a large baby. This was performed with no complications other than being unable to bear weight postoperatively. Her medical history included schizophrenia and gestational diabetes. She was taking antipsychotic medications in the form of sodium valproate, aripiprazole and fluoxetine. She was also taking insulin during her pregnancy. She did not consume alcohol and was a non-smoker.
On examination, her right hip was shortened and externally rotated with no active range of movement due to pain. Her left hip had no pain on palpation or on movements. Both lower limbs were neurovascularly intact.
Investigations
An X-ray of the hip and pelvis was carried out postnatally (figures 1 and 2). This revealed a displaced right femoral neck fracture. Subsequently, an MRI scan was performed to investigate the nature of the atraumatic fractures (figures 3 and 4). This confirmed the diagnosis as well as identifying an undisplaced left femoral neck fracture. Postoperatively, the patient was investigated with a DEXA scan revealing severe osteoporosis (T-score and Z-score −3.7 at the lumbar spine). Blood results revealed normal renal function, calcium, vitamin D, phosphate, magnesium, thyroid and parathyroid function tests.
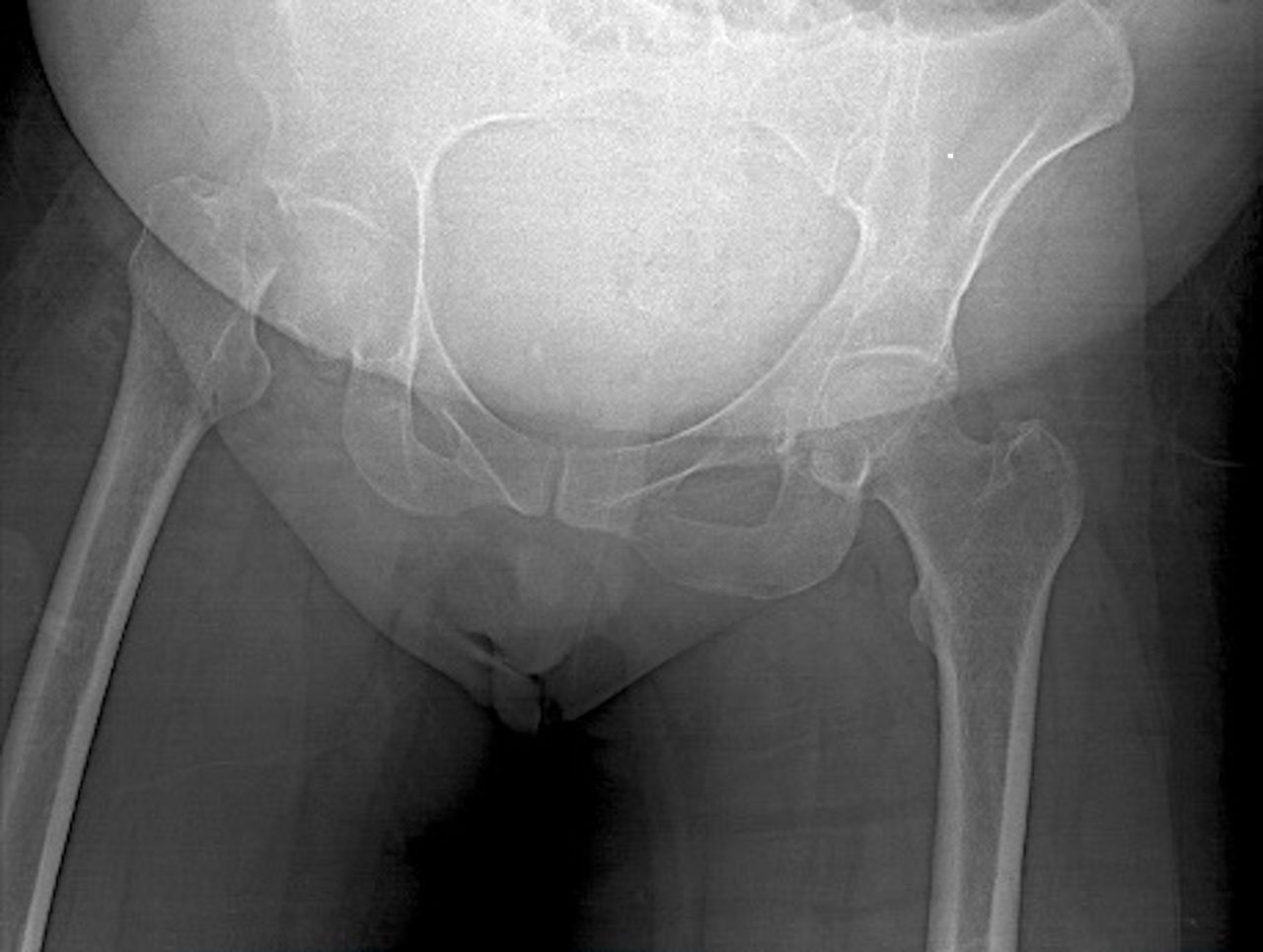
Anteroposterior X-ray obtained on presentation showing right intracapsular neck of femur fracture.
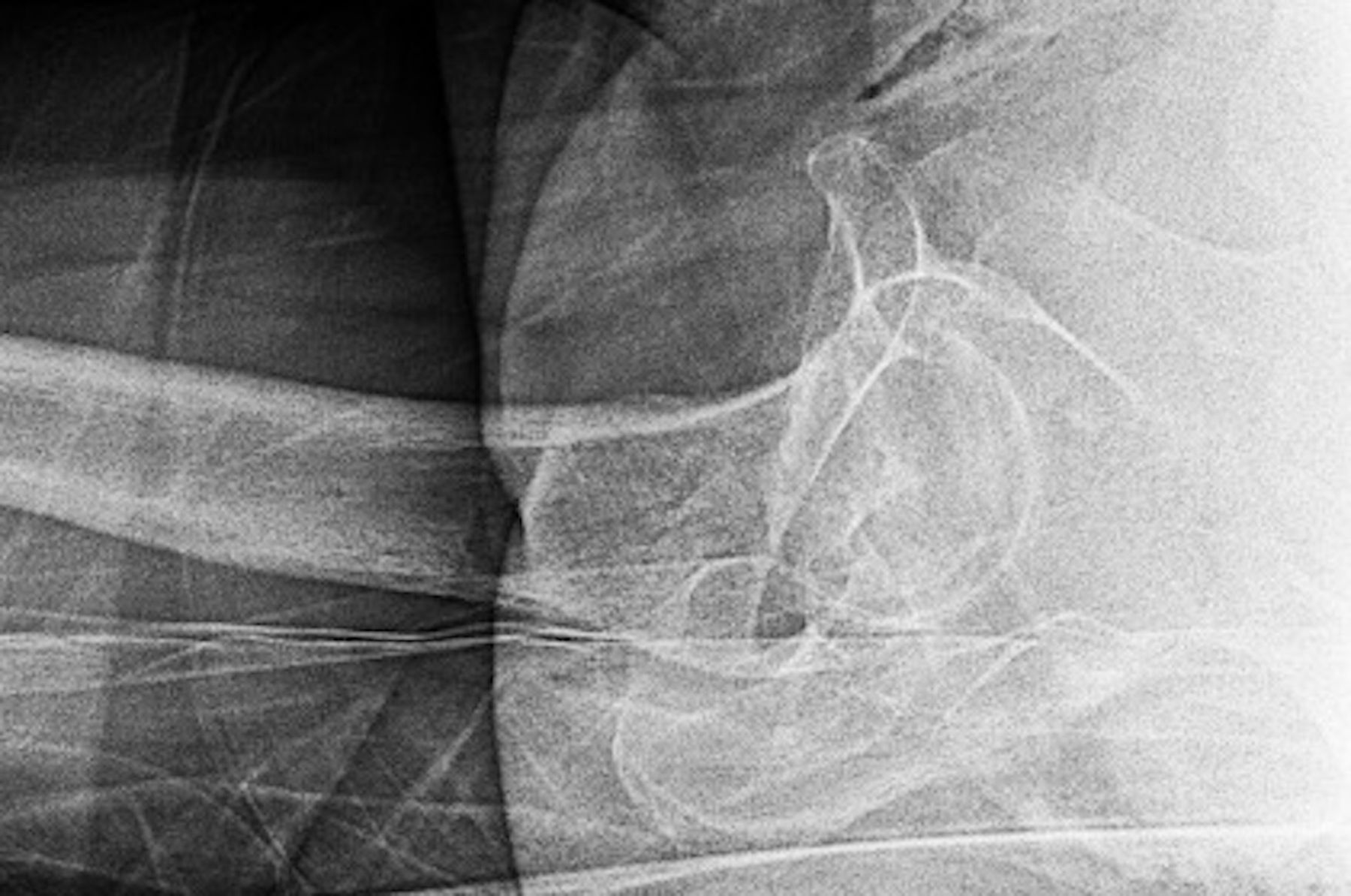
Lateral X-ray of right intracapsular neck of femur fracture.

T1-weighted coronal MRI showing hypointense signals in the right and also left femoral necks confirming bilateral intracapsular hip fractures.

T1-weighted short tau inversion recovery (STIR) coronal MRI showing hyperintense signals in the right and left femoral necks revealing fractures.
Treatment
Consensus opinion from a wider group of hip surgeons within the region was sought due to the rarity of this problem and the patient’s young age. A decision was made to perform a right total hip replacement and left dynamic hip screw fixation (figures 5 and 6). The operation would offer the benefit of allowing the patient to bear weight immediately, and a dynamic hip screw would stabilise the left hip, preventing displacement, and allow healing to reduce the risk of avascular necrosis. A ceramic on polyethylene bearing surface was used to avoid the possible exacerbation of the patient’s auditory hallucinations from the potential squeaking of a ceramic-on-ceramic surface. Both procedures were performed under the same anaesthetic 3 days following her caesarean section. The patient was able to mobilise, bearing full weight with crutches postoperatively and was discharged with outpatient follow-up from the orthopaedic, obstetric and endocrinology teams. She was given calcium and vitamin D supplementation by the bone metabolism team and is being considered for bisphosphonate therapy.

Postoperative anteroposterior X-ray of right total hip replacement (THR) and left dynamic hip screw (DHS).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Postoperative lateral X-ray of right THR.
Outcome and follow-up
The patient was followed up at 6 and 12 weeks postoperatively. At her most recent appointment, she was managing to fully bear weight without any mobility aids, and her radiographs showed no evidence of avascular necrosis. She will also have a repeat bone scan and be followed up by the bone metabolism clinic at 1-year postdischarge.
Discussion
The incidence and mechanism of TOH are unknown. Some women may have a low peak bone mass or be in an accelerated bone resorptive state prior to conception, and pregnancy allows it to become clinically obvious. In some reported cases, there are other secondary causes of osteoporosis including chronic heparin, anticonvulsant or corticosteroid use, suggesting pregnancy may not be solely to blame.1 Our patient was also on regular antipsychotic medication, and these have been linked to hyperprolactinaemia which can lead to reduced bone mineral density (BMD) and osteoporosis.2 There have also been documented cases of TOH where the female child resulting from the pregnancy has been found to have low BMD in childhood. This suggests there may be a genetic element. This was our patient’s first pregnancy; however, whether increased parity has a negative or beneficial impact on BMD or risk of fracture is inconclusive. In our patient, the combination of her antipsychotic medication, diabetes and her genetic composition is all likely to have contributed to this complication of TOH.
Pregnancy and lactation create a change in bone metabolism. Calcium is required for fetal growth and lactation. The increased calcium demand on top of hypoestrogenaemia during pregnancy can lead to bone mineral loss and is therefore contributory in the development of TOH. One study found a 7.6% bone density loss at the lumbar spine immediately post partum compared with age-matched, non-postpartum controls.3 To compensate for the raised calcium demand, particularly during the third trimester, the intestinal absorption of calcium during pregnancy doubles.4 However, studies found that all markers of bone turnover increased during pregnancy and failed to return to normal baseline levels by 12 months post partum, suggesting maternal skeletal stores are also depleted to compensate.5 Additionally, the change in hormone levels such as progesterone, oestrogen and relaxin can lead to ligament laxity. The 10–15 kg weight gain can increase bone and joint loading during everyday activities. Women often undergo less physical activity during pregnancy, particularly during the third semester.6 Additionally, conditions such as pregnancy-induced hypertension or preterm labour can lead to women being on long-term bed rest. These factors can all contribute to increasing the risk of stress or fatigue fractures during labour.
As lactation increases calcium demands and produces hormonal changes, studies have looked into lactation-related bone losses, but the results vary substantially. Some studies suggest a >5% loss of BMD within the spine due to breastfeeding, but the quantity of bone loss is positively associated with the volume of breast milk produced. However, this loss appears to be transient as there is full recovery following cessation of lactation. Alongside weaning, return of menstruation and use of progesterone-only pill were associated with improved recovery.6
Fragility fractures often occur in the first pregnancy, commonly in the third trimester or in the first month post partum, often in the spine or hips. Patients most frequently present with the multiple vertebral fractures. The increased BMD loss in the spine compared with the hip is thought to be a result of bone composition: vertebrae are rich in trabecular bone which has a higher turnover rate, while the hip has more cortical bone.7 This is reflected in a study comparing BMD loss in hip and spine during pregnancy where the T-scores and Z-scores were higher at the hip than the spine regardless of maternal age, parity and/or lactation history.8 Our patient underwent a bone scan postoperatively which only included the lumbar spine due to the bilateral hip implants, and therefore a comparison of bone density between hip and spine was not possible.
Early diagnosis is key to prevent serious complications and should be considered in pregnant patients presenting with persistent hip or lower back pain. If suspected, MRI is the imaging modality of choice. Identifying fractures in the acute stage before they become displaced or result in avascular necrosis affects the long-term impact on the patient. Any fracture identified will require an operation to internally fix the bone or even replace the joint altogether if avascular necrosis is a risk.
There are currently no guidelines in terms of prevention; lifestyle changes are a good first step: sufficient exposure to sunshine for vitamin D and regular exercise to help strengthen bones. Vitamin supplements can also play a key role.7 The current guidance for daily calcium intake for non-pregnant individuals is 700 mg.9 Recommendations for daily vitamin D is 400 IU and includes those who are pregnant.10 The condition can be pharmacologically managed with bisphosphonates. One study has shown a substantial increase of 23% in spinal BMD in response to early bisphosphonate therapy alongside calcium and vitamin D supplementation. In individuals without bisphosphonate therapy, the spinal BMD increase was 11%.11 There is no clear optimal duration for bisphosphonate therapy following birth, although 5 years seems to be widely accepted.4 11 However, there are concerns about bisphosphonates collecting within the maternal bone and being exposed to the fetus of subsequent pregnancies, affecting the fetal skeletal development.4 Teriparatide, a parathyroid hormone treatment, has been recently proposed as an alternative treatment. It has been shown to increase BMD and reduce the risk of osteoporotic fracture. Following 13 months of treatment with teriparatide, one study demonstrated a 24.4% increase in lumbar spine BMD and 12.6% and 7.8% at the left and right neck of femur, respectively.12 Furthermore, it does not accumulate in the maternal skeleton and does not affect a future fetus after cessation of therapy.
A previous case report documented a woman of similar age to our patient who presented with increasing pain in her right leg at 30 weeks’ gestation. On presentation, she underwent an MRI scan which revealed TOH and a stress fracture. To reduce the risk of hip fracture, the patient was put on bed rest for the remainder of her pregnancy and underwent a caesarean section to avoid a vaginal birth. Postnatally, the patient was given vitamin D replacement and bisphosphonates; by 6 months post partum, her symptoms and MRI changes had resolved. This case demonstrates the importance of early recognition of TOH.13
In summary, women with TOH often suffer severe and disabling back/hip pain. Exact mechanisms involved are still debated, and there are many factors that increase the risk of reduced BMD during the pregnancy and lactation period. Having a low index of suspicion in patients with disproportionate pelvic or hip pain will allow early identification of possible fractures. MRI scanning is the recommended method of investigation during pregnancy. MRI is safe during the second and third trimesters of pregnancy, and while consideration should be given to use in the first trimester, there are no associated long-term complications.14 This is vital to initiate treatment promptly and reduce the risk of complications, such as avascular necrosis.
Learning points
The exact mechanisms involved in transient osteoporosis of the hip (TOH) are still unclear, and aetiology is multifactorial.
We know there is higher risk of reduced BMD during the pregnancy and lactation period.
Early identification is crucial as there are treatment options available that reduce the risk of fracture.
Clinicians should have a low index of suspicion for investigating TOH in pregnant patients who present with severe back or hip pain.
Ethics statements
Patient consent for publication
Footnotes
Twitter @sooryasiva5
Contributors SS: submitting author, involved in writing this case report. QL: orthopaedic registrar, involved in the management of case and writing this case report. AA: consultant orthopaedic surgeon, involved in management of this case. KP: consultant orthopaedic surgeon, provided expert opinion on management of case and involved in editing and reviewing this case report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.