Article Text

Abstract
Strongyloidiasis is a disease caused by the intestinal helminth Strongyloides stercoralis. When the immune system of infected individuals is compromised, larvae may migrate from the gastrointestinal tract to other tissues, causing S. stercoralis hyperinfection syndrome, which has a reported mortality of 71%. In this case, we report a patient with S. stercoralis hyperinfection syndrome with central nervous system (CNS) involvement. An elderly South East Asian male tourist presented with pulmonary symptoms, fever and infiltrates on chest X-ray. He later developed symptoms of CNS infection. S. stercoralis larvae were found in a stool sample. Microbiological examination of cerebrospinal fluid revealed S. stercoralis-specific DNA. The patient was treated with oral and rectal ivermectin and albendazole. The condition was complicated by sepsis, bacteraemia and hypereosinophilia. Unfortunately, the patient eventually died from pulmonary oedema and insufficiency. This case highlights the global importance of Strongyloides CNS infection in endemic and non-endemic regions.
- Infectious diseases
- Tropical medicine (infectious disease)
- Travel medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Strongyloidiasis is a common disease in the tropics and subtropics and is caused by the intestinal helminth Strongyloides stercoralis. This nematode is remarkable in its capacity to complete its lifecycle completely both inside and outside the host. In the host, the infection is usually initiated by filariform larvae penetrating intact skin. The larvae migrate through the alveoli to the respiratory tract and are swallowed and passed to the small intestine where they mature and deposit eggs in the intestinal mucosa. The eggs are then either excreted in the faeces or they hatch into rhabditiform larvae, changing into the infective filariform stage, which can reinfect the host by penetrating the bowel or the perianal skin. They can thus cause an autoinfection, which may last for several years, possibly decades.1 The lifecycle of S. stercoralis is shown in figure 1.2 Between 10% and 40% of the population in tropical and subtropical areas might be infected by S. stercoralis.3 In migrants from East Asia, the seroprevalence is 17.3%, and the prevalence based on detection of the larvae in stool is 3.9%.4 5 The estimated global prevalence of S. stercoralis is shown in figure 2.6 In immunocompromised individuals, the filariform larvae can disseminate to any organ, causing hyperinfection with a reported mortality of 71%.7 8 S. stercoralis hyperinfection syndrome may be seen in patients with human T-cell lymphotropic virus type 1 or HIV/AIDS, patients suffering from malignant neoplasm, individuals with alcohol abuse, transplant patients and in patients treated with corticosteroids.1 9 10
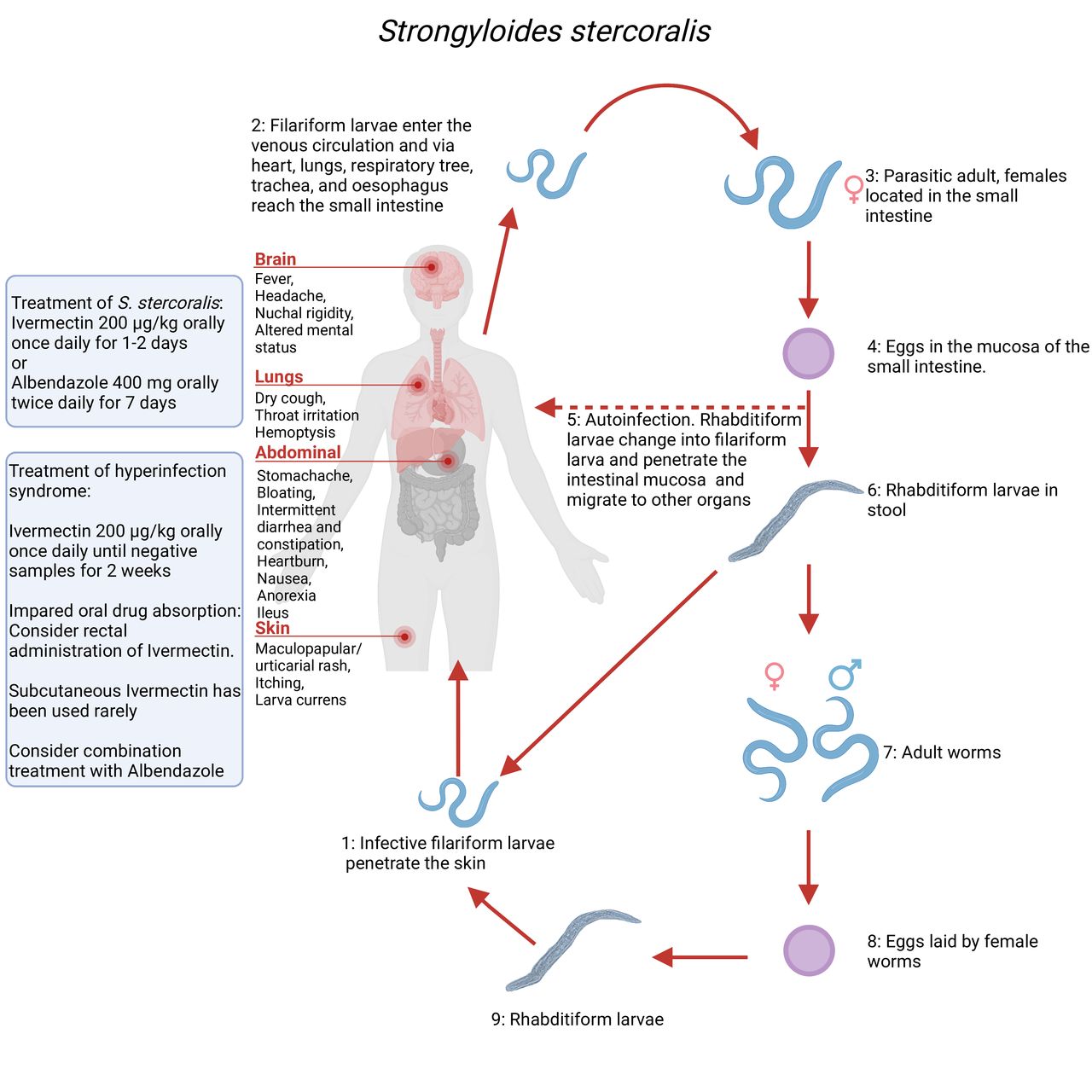
The lifecycle of Strongyloides stercoralis. 1: The infective filariform larvae begin the parasitic cycle by penetrating the skin. 2: The larvae migrate to the small intestine either via connective tissue, viscera or by migrating through lymphatic system to lungs, where they are coughed up and swallowed. 3 and 4: Female worms lay eggs in the mucosa of the small intestine. 5: Larvae penetrate from the intestinal mucosa and migrate to other organs causing autoinfection. 6: Rhabditiform larvae are excreted in the stool and either develop into infective filariform larvae (1) or enter the free-living cycle. 7: The larvae mature into adult worms. 8: The worms lay eggs, which hatch into rhabditiform larvae. 9: The larvae develop into infective filariform larvae, which can penetrate the skin.2 The common symptoms of infection and treatment suggestions are provided on the left. Created with www.BioRender.com by AAP.
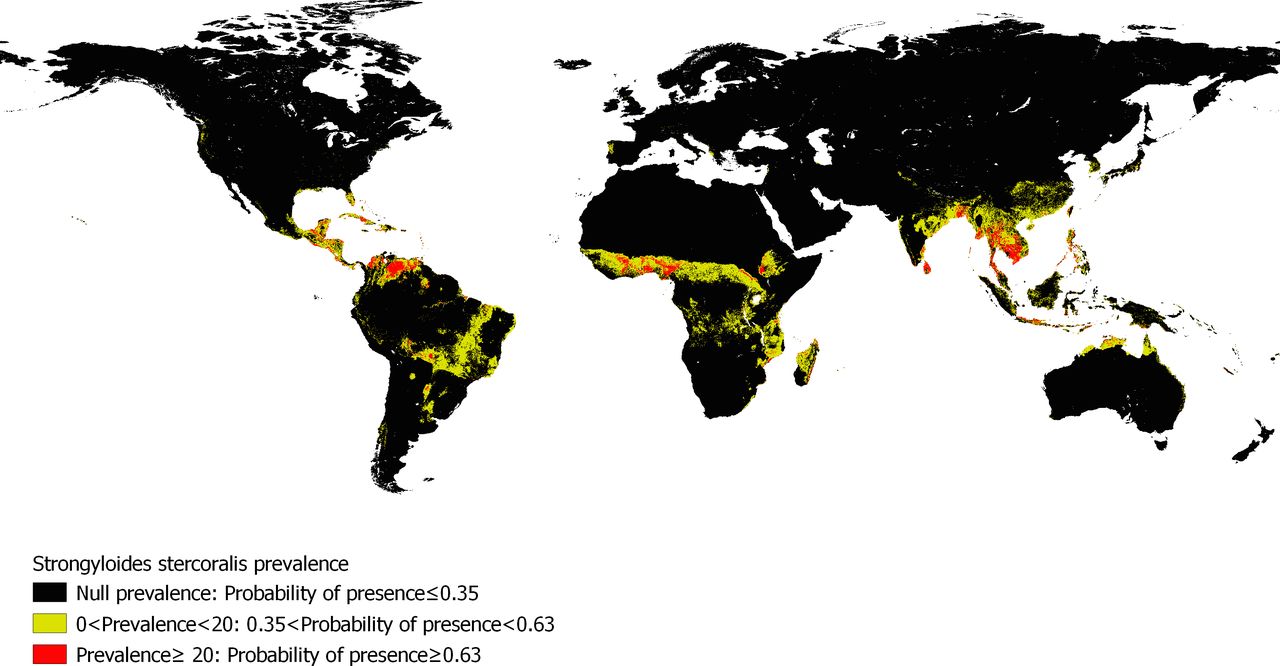
Map of the estimated prevalence of Strongyloides stercoralis as published in Fleitas et al CC BY 4.0.6
Here, we report a case of primary S. stercoralis central nervous system (CNS) infection, which is a rare manifestation of S. stercoralis hyperinfection syndrome.
Case presentation
A South East Asian man in his 70s presented with cough and purulent sputum. His medical history included hypertension, myocardial infarction, nephrolithiasis and surgical stone extraction. He was a former smoker (30 pack-years) and reported no alcohol use. He was born and raised in South East Asia.
Six days after arrival, he complained of productive coughing, fever and was seen by a general practitioner and treated with phenoxymethylpenicillin for pneumonia (day 0). He was admitted to the emergency department on day 8 due to fever, malaise, nausea and headache. The physical examination revealed diffuse abdominal tenderness, normal chest auscultation and a few skin excoriations on his extremities. No other skin changes were noted. Again, he was treated for pneumonia based on the presence of bilateral infiltrates on chest X-ray (figure 3). Blood eosinophils were 2.46×109/L on admission. He was discharged on day 9 after overall improvement. On day 15, he was readmitted due to new-onset seizures. Neurological examination was normal, and no skin changes were noted. CT scan of the head showed a small hypodense area in the corona radiata, interpreted as sequelae of cerebral infarction. The seizures were thus thought to be postinfarction seizures, and antiplatelet therapy was initiated. On day 52, he was readmitted to the emergency department with severe abdominal pain and fever. The blood eosinophil counts were 0.05×109/L (figure 4). A distended and tender abdomen was found on physical examination. A CT scan of the abdomen revealed severe coprostasis and an oedematous caecum. He received empirical antibiotic treatment with piperacillin/tazobactam. The next day, his condition worsened with the development of a severe headache and nuchal rigidity. Lumbar puncture was performed, showing pleocytosis with 1300×106/L cells (920×106 polymorphonuclear and 420×106 mononuclear cells), a glucose level of 3.6 mmol/L and a protein level of 3.55 g/L in the cerebrospinal fluid (CSF).
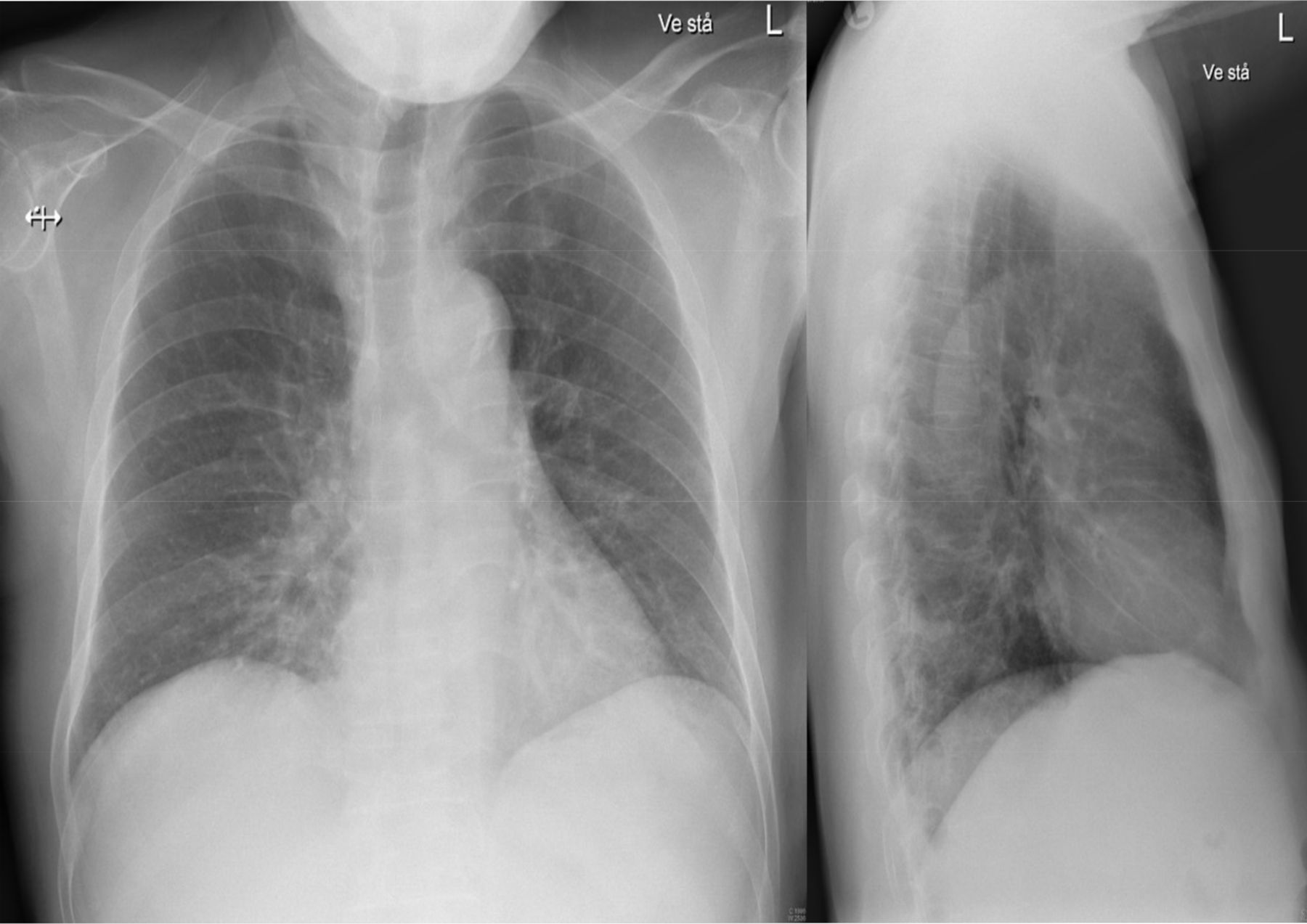
Thoracic X-ray at first admission. Anterior-posterior (left) and lateral view (right) showing bilateral basally located pneumonic infiltrates, most markedly on the right side. The patient was initially treated for pneumonia based on this presentation.
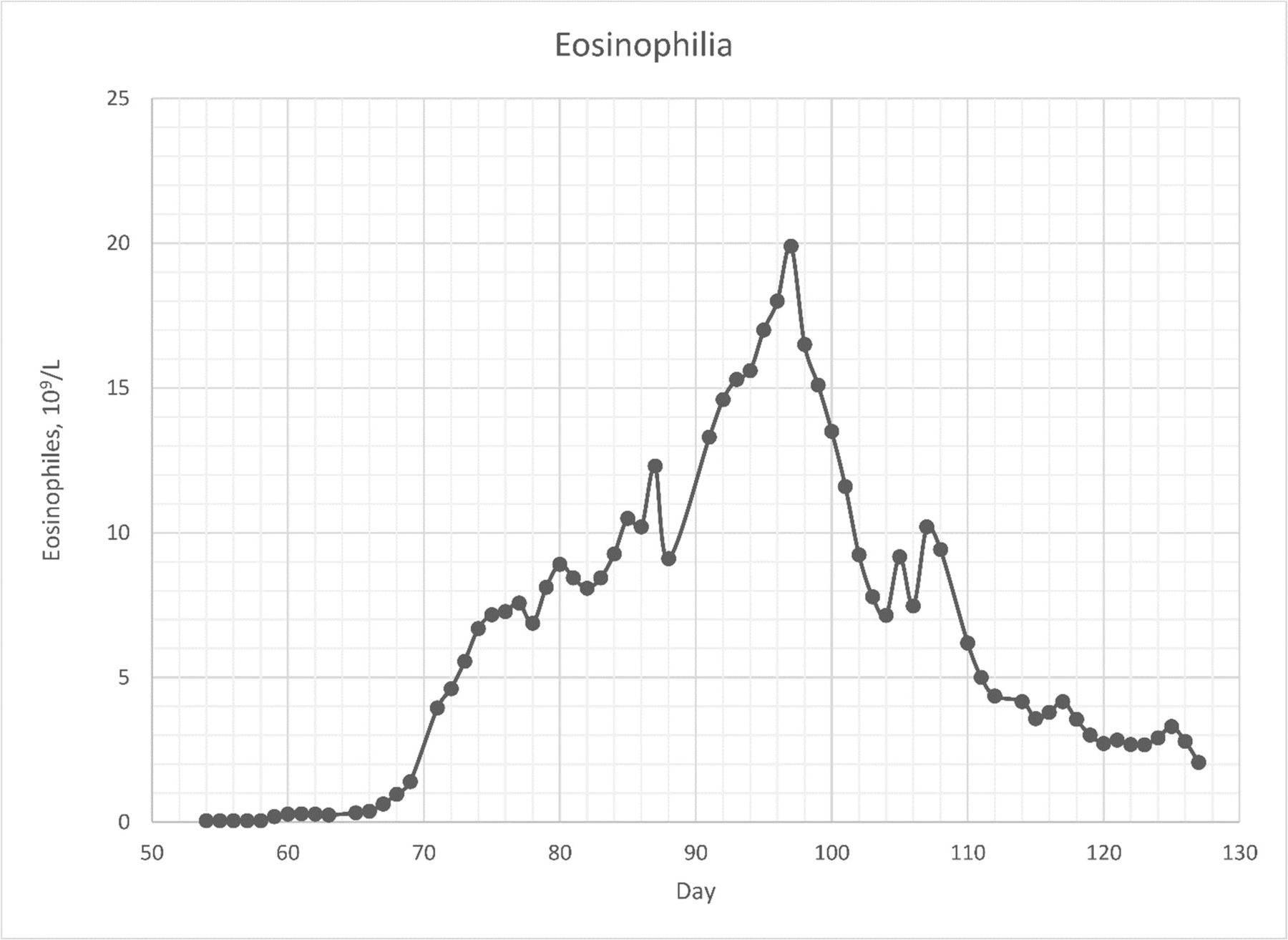
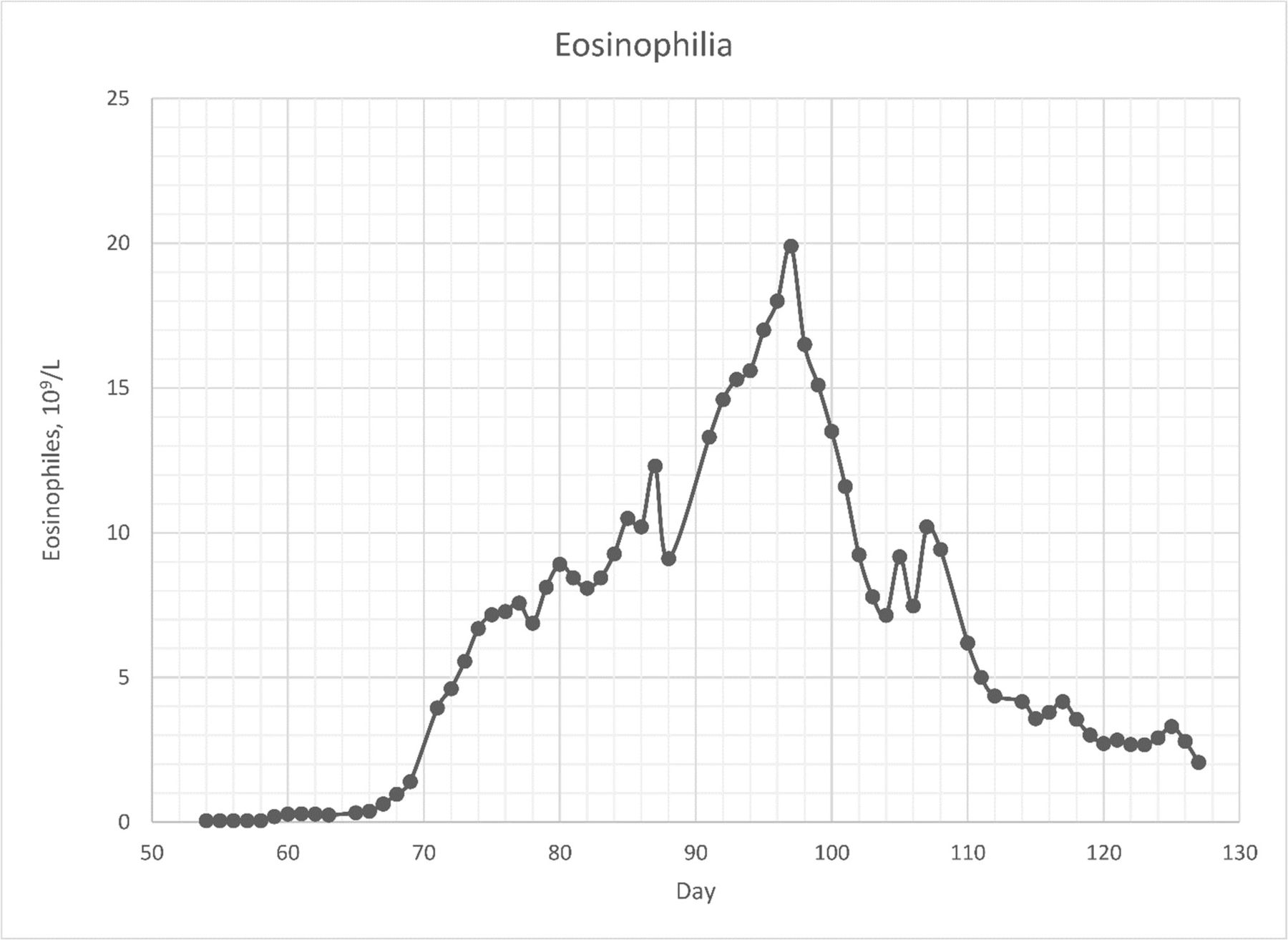
Time course of the blood concentration of eosinophils (×109/L). Graph created by AAP.
Investigations
CSF analyses with multiplex PCR in the FilmArray meningitis/encephalitis panel (BioFire Diagnostics, Salt Lake City, Utah, USA) were negative. Blood and CSF cultures were also negative. The patient was treated with benzylpenicillin, ceftriaxone and dexamethasone based on a presumptive clinical diagnosis of bacterial meningitis. A brain MRI scan showed a probable empyema in the right hemisphere. Stool samples were tested for pathogenic bacteria, virus and parasites. Microscopy of the stool revealed S. stercoralis rhabditiform larvae (figure 5). The blood eosinophil count continued to rise during the initial phase (figure 4). Analysis of bacterial, fungal and parasitic DNA (16S and 18S ribosomal RNA analysis) in the initial CSF sample revealed S. stercoralis-specific DNA.11 This was confirmed by targeted real-time PCR-based detection of S. stercoralis DNA. Furthermore, the patient tested positive serologically with a strong anti-Strongyloides antibody reaction by an enzyme-linked immunosorbent assay (Strongyloides ratti No. 9450, Bordier Affinity, Switzerland).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Filariform larvae of Strongyloides stercoralis observed by microscopy of a stool sample from the patient. The short buccal cavity characteristic of S. stercoralis is visible.
Differential diagnosis
Comprehensive investigations during hospitalisation were carried out to rule out underlying malignancy, primary and secondary immunodeficiencies, rheumatological diseases and other infectious diseases. Tests included positron emission tomography-CT, and multiple CTs of the brain, thorax and abdomen, bone marrow microscopy, blood smear, immunoglobulins (IgA, IgM, IgG, IgG1, IgG2, IgG3, IgG4 and IgE), lymphocyte populations (CD19+, CD3+, CD4+, CD8+ and CD3–CD16/CD56+), M-protein, antinuclear antibodies, antineutrophil cytoplasmic antibodies and serology for human T-cell lymphotropic virus type 1 and 2, HIV, syphilis and viral hepatitis. The tests were unremarkable, except for a slightly elevated total IgG and a haemoglobin A1c (HbA1c) concentration of 70 mmol/mol (8.6%) with an average glucose level calculated at 10.9 mmol/L, which meets the diagnostic criteria for new-onset type 2 diabetes mellitus. However, the HbA1c was performed 11 days after administration of dexamethasone, which could have altered the HbA1c levels and thus the reliability of the diagnosis. The patient had no haemoglobinopathy and did not receive treatment with corticosteroids prior to admission.
Treatment
A diagnosis of Strongyloides hyperinfection with CNS involvement was made, and the patient was treated with oral ivermectin 200 µg/kg once daily for 37 days and albendazole 400 mg two times per day for 24 days. Rectal ivermectin and albendazole equivalent to the oral dose were given initially during the first 16 days due to paralytic ileus and potentially impaired oral drug absorption in the intestinal tract.
Outcome and follow-up
Subsequent analysis of the CSF obtained 28 days after the initial lumbar puncture tested negative for both Strongyloides-specific real-time PCR and 16S and 18S ribosomal DNA analyses. S. stercoralis culture (‘filter paper method’) was used to evaluate treatment response, and no larvae were grown from the stool after treatment initiation.
The condition was complicated by Klebsiella pneumoniae sepsis, catheter-associated Staphylococcus epidermidis and Staphylococcus haemolyticus bacteraemia and a marked hypereosinophilia with a peak of 19.9×109/L (figure 4). Unfortunately, the patient died from pulmonary oedema and pulmonary insufficiency 82 days after the last admission and 20 days after testing negative for Strongyloides-specific DNA in the CSF.
Discussion
Strongyloides infection in the CNS has been reported previously, although almost exclusively in immunocompromised patients.12–17 Strongyloides seropositivity has been positively associated with diabetes, and few cases of disseminated strongyloidiasis associated with diabetes in the absence of any major immunodeficiency have been reported.7 18 19 On the other hand, animal studies of helminth infections have shown a positive effect on glucose metabolism.20 However, the ability to clear or control strongyloidiasis might be impaired in patients with type 2 diabetes.18 We present a case of CNS-involving strongyloidiasis in a patient with undiagnosed type 2 diabetes.
Strongyloides is prevalent in the tropics and subtropics, and even though the global prevalence is unknown, it is estimated that 30–100 million persons are infected worldwide.2
The seroprevalence in the adult population in regions of South East Asia is high (12.1%).5 21 However, the CNS manifestation of strongyloidiasis is extremely rare—even more so in non-endemic countries, where only eight antemortem cases have been documented.13 17 22–27 In the majority of cases, patients have a compromised immune system, for example, due to corticosteroid therapy, malignancy or chemotherapy. The prognosis of disseminated strongyloidiasis with CNS involvement is poor and associated with high mortality. Most cases of strongyloidiasis involving the CNS are diagnosed only on autopsy. Treatment of S. stercoralis infection is challenging due to the lack of sufficient evidence. Two doses of ivermectin 200 µg/kg orally 14 days apart have has previously been recommended.28 However, in uncomplicated infections, it is debated whether a single dose of ivermectin 200 µg/kg is as efficient as two or four doses of 200 µg/kg given on days 1, 2, 15 and 16.29 30 In hyperinfection/disseminated disease, ivermectin 200 µg/kg once daily continued for 14 days after the demonstration of negative stool samples for larvae has been suggested, often combined with empirical antibiotics targeting enteric pathogens.8 Alternatively, ivermectin can be combined with albendazole.29 31 A parenteral formulation of ivermectin for subcutaneous use in animals (Ivomec vet 1% injection) has been suggested for patients who do not tolerate oral therapy.8 32
Treatment of CNS-involving strongyloidiasis still relies on limited evidence. In one case, successful treatment was achieved using 400 mg albendazole two times per day for 3 months.13 In another report, treatment with ivermectin 200 µg/kg once daily resulted in clearance of larvae from CSF; however, the patient died from cerebral damage.17 A combination of ivermectin and albendazole has also been used in two cases with favourable outcomes.12 In our case, the patient achieved CSF clearance after combined treatment with ivermectin and albendazole, although he, unfortunately, died later in the course of hospitalisation due to respiratory insufficiency.
In conclusion, we report a case of Strongyloides hyperinfection presenting with pulmonary symptoms and meningitis in a South East Asian immunocompetent adult patient with type 2 diabetes. The patient was seen several times with pulmonary symptoms misdiagnosed as community-acquired pneumonia before he developed Strongyloides-induced meningitis. This case highlights the importance of a high degree of clinical suspicion required for the diagnosis of Strongyloides CNS infection in patients from endemic areas, owing to the high mortality. The disease should be suspected in patients from endemic areas who present with neurological and respiratory symptoms.
Learning points
Strongyloides can cause autoinfection (filariform larvae migrate from the large intestine to infect other organs) lasting for several years, and the disease is very common in the tropical and subtropical areas.
Strongyloides hyperinfection often affects immunocompromised patients and can cause severe disease with high mortality.
Strongyloides hyperinfection can manifest with symptoms corresponding to the affected organs, for example, fever, dry cough, throat irritation (lungs), stomachache, bloating, intermittent diarrhoea and constipation, heartburn, nausea, loss of appetite (gut), headache, nuchal rigidity and altered mental status (central nervous system).
Treatment options include oral and/or rectal ivermectin and/or albendazole; however, the better choice is still debated.
Diabetes may increase the risk of Strongyloides hyperinfection; however, the precise relationship between the two conditions is yet to be established.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors AAP and RMI conceptualised the report and collected clinical data. CRS was responsible for the PCR tests of Strongyloides stercoralis. GNH was responsible for the S. stercoralis microscopy. AAP drafted the manuscript. All authors critically revised the manuscript and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.