Article Text

Statistics from Altmetric.com
Description
Bruck syndrome is an autosomal recessive disease characterised by the clinical combination of both osteogenesis imperfecta and arthrogryposis multiplex congenita (AMC). It is caused due to collagen miss-folding and cross-linking defect resulting from a deletion in FKBP10 (OMIM #259450) and/or PLOD2 (OMIM #609220) gene.1 2 This disorder is an extreme rarity and the reported incidence rate is less than one in a million and to the best of our knowledge, less than 40 cases are reported in the existing medical literature.3
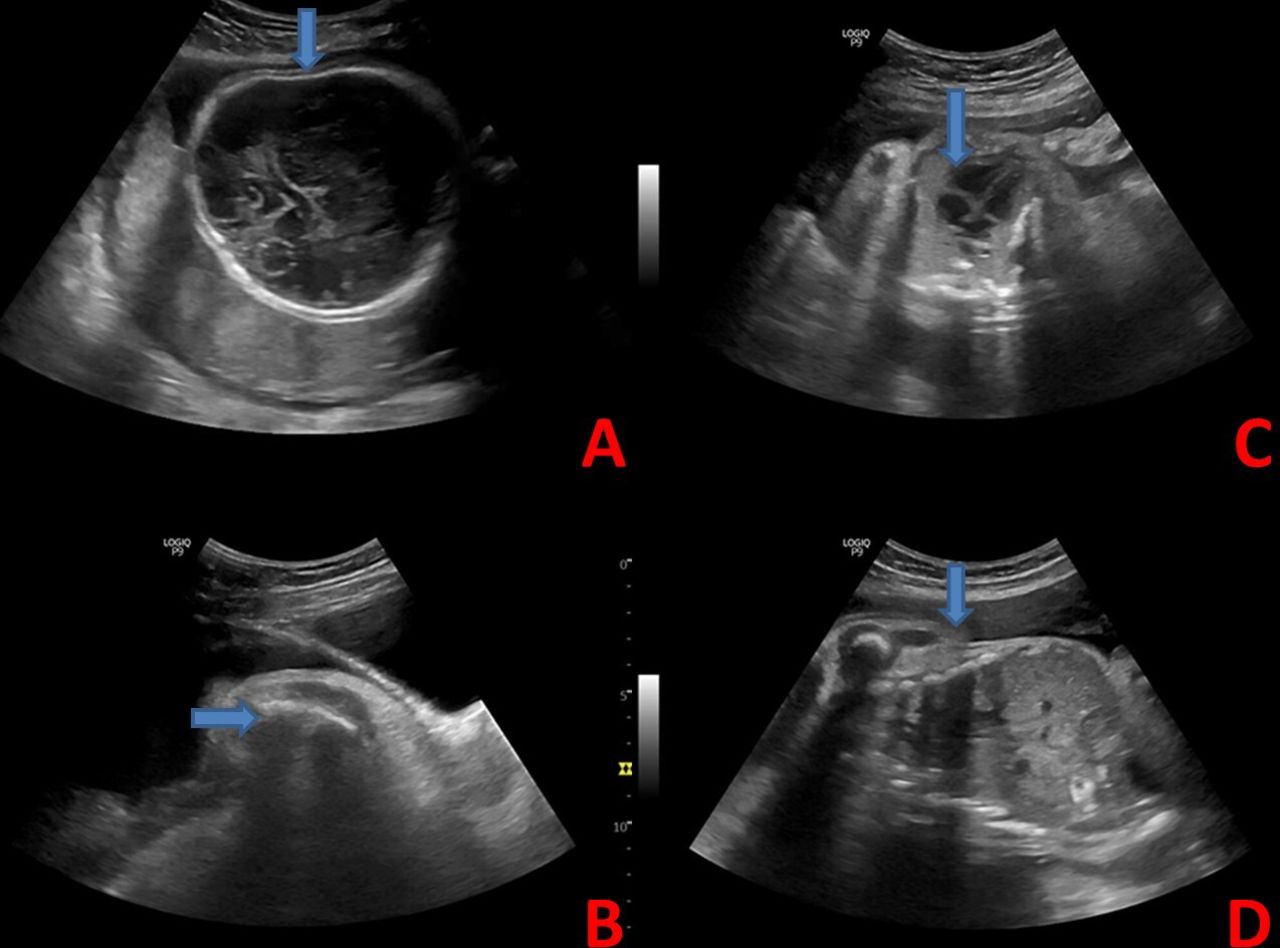
Herein, we report a 19-year-old primigravida at 38 weeks period of gestation (according to last menstrual period) who presented in the obstetrics emergency room with decreased fetal movements since last 12 hours. The parents denied consanguinity. There was no significant family history of a baby born with skeletal dysplasia or gross congenital anomaly. Previous antenatal scan at 19 weeks 6 days period of gestation showed single live intrauterine fetus with biparietal diameter: 50 mm (corresponding to 19 weeks 6 days), head circumference: 177 mm (corresponding to 20 weeks 1 day), abdominal circumference: 139 mm (corresponding to 19 weeks 6 days), femur length: 19 mm (corresponding to 16 weeks 0 day) and amniotic fluid index (AFI): eight (adequate). At this time, no abnormal shape of the femur was noted. A 4D ultrasonography (USG) was advised for fetal anomaly detection, but the patient did not undergo the scan. General physical examination was unremarkable. Obstetric examination revealed a gravid uterus corresponding to 30 weeks. Transabdominal ultrasound revealed a single live intrauterine fetus with softened calvaria possibly decreased calvarial ossification (figure 1A), curved, shortened and beaded appearance of all the long bones (figure 1B), triangular thoracic cavity and narrowed pelvis (figure 1C,D). The gestational age at this point could not be determined accurately with USG as the femur appeared short and curved, possibly due to multiple fractures and hence the femur length could not be measured. Although the biparietal diameter corresponded to 31 weeks 3 days (83.1 mm), head circumference corresponds to 31 weeks 5 days (286 mm) with adequate liquor (AFI-10). Our provisional diagnosis was osteogenesis imperfecta. In view of the non-reassuring non-stress test, a decision for the lower segment caesarian section was taken. The baby was delivered (birth weight: 1.89 kg) with multiple joint contractures specially fixed flexion deformity of the elbow, wrist and hip and extension of the knee joint (figure 2A). Although the baby died within 2 hours after birth despite resuscitative measures. Postmortem neonatal X-ray showed short, broad curved long bones, angulation of the tibia, multiple fractures and incomplete beading of ribs (figure 2B,C). We clinically concluded that this was a case of osteogenesis imperfecta type 2B associated with features of AMC which is nothing but Bruck syndrome. We also considered Jeune syndrome as a differential diagnosis that consists of a narrow chest, short broad ribs and shorten bones in arms and legs. Although polyhydramnios was absent in our case. To confirm the diagnosis and counsel the parents regarding future pregnancy, genetic testing was warranted. After taking informed consent, genetic testing was done, which showed defects in the PLOD2 gene, homozygous mutation: c.797G>T, p.Gly266Val. Heterozygous mutations of the PLOD2 gene were also detected in both parents. As this is an autosomal recessive disorder, with both parents being carriers, there is a 25% chance that the offspring will be diseased. Hence a prenatal diagnostic modality was adviced for future pregnancy. We also advised genetic testing for the siblings of carrier parents to prevent recurrence in the community.
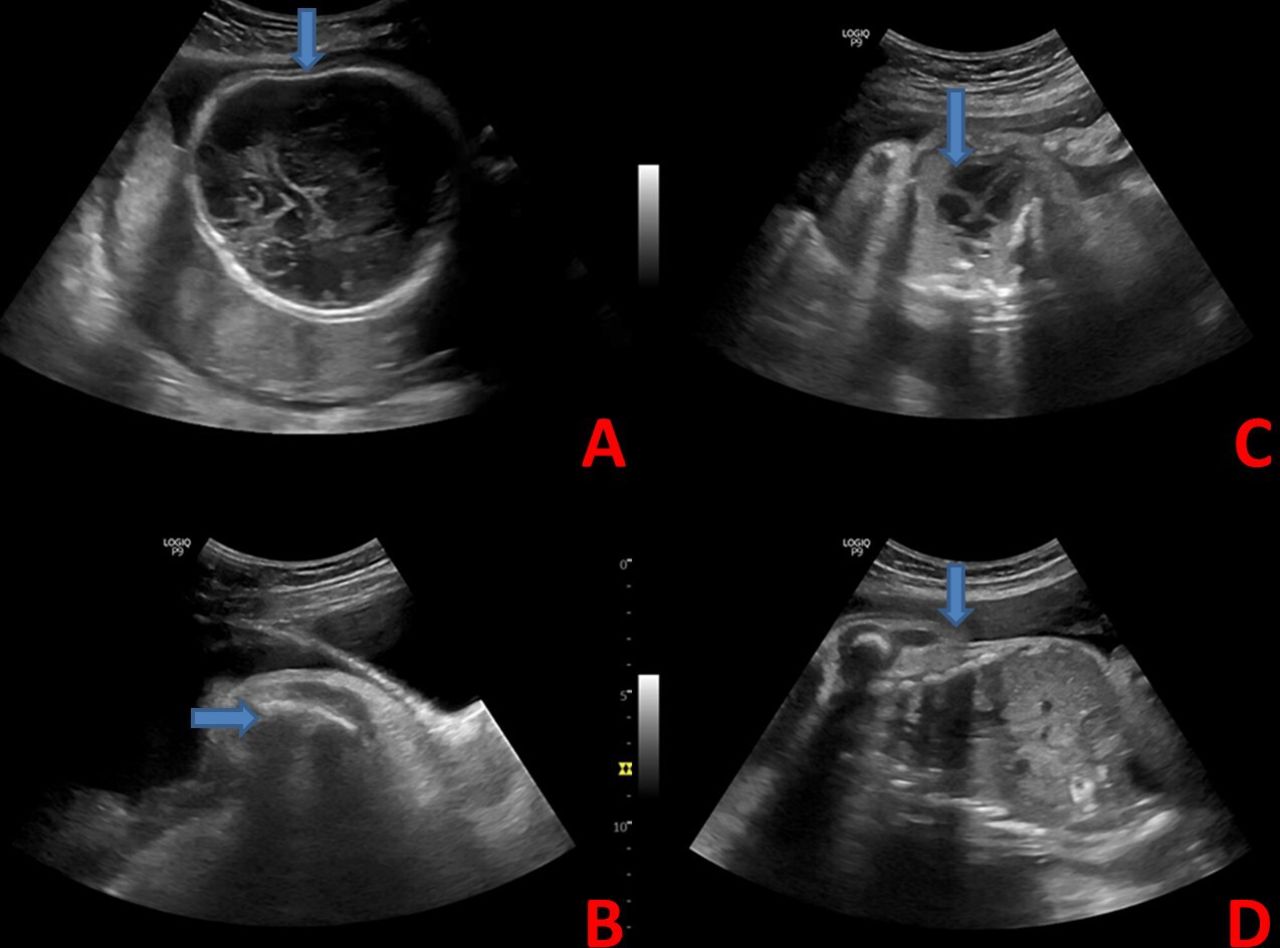
Antenatal transabdominal ultrasound showing: (A) compressible fetal skull with transducer, (B) shortened and angulated long bones with evidence of fracture, (C) narrowed thoracic cavity occupied by heart and (D) narrowed pelvis.

{kind=link}
{kind=link}
(A) Neonate with multiple joint contractures; specially fixed flexion deformity of the elbow, wrist and hip and extension of the knee joint, (B) chest X-ray showing ribs with incomplete beading and (C) X-ray showing short, broad, crumpled long bones along with angulation of tibia.
Besides reporting a very rare clinical entity, the main purpose of reporting this case was to make the readers aware that whenever one comes across a neonate with features suggestive of AMC, radiological assessment should be done immediately to rule out underlying osteogenesis imperfecta.4 If a fetus is seen to have features suggestive of AMC and osteogenesis imperfecta, one should consider Bruck syndrome. This will not only provide an accurate diagnosis but also help in educating the caregivers regarding preventive measures like gentle handling, padding of beds, etc to prevent further fractures. Routine orthopaedic consultation would be required for these patients to help them in rehabilitation. Although in our case the patient presented to us quite late for prenatal diagnosis and successive line of management, prompt assessment of bony abnormalities or AMC should be done to look for potential causes as rarely do they have a good long-term outcome.
Learning points
Bruck syndrome can be detected antenatally and it can be rare differential of reduced fetal movements.
Osteogenesis imperfecta should be routinely ruled out in all cases of arthrogryposis multiplex congenital.
Caregivers should be educated regarding the preventive measures like gentle handling, padding of beds, etc to prevent further fractures in a case of Bruck syndrome.
Ethics statements
Patient consent for publication
Footnotes
Contributors SP: Conception, design of the study, acquisition of the data, drafting the manuscript, final approval of the version to be submitted. DNB: Conception, design of the study, acquisition of the data, drafting the manuscript, final approval of the version to be submitted. AD: Acquisition of the data, final approval of the version to be submitted. SR: Acquisition of the data, final approval of the version to be submitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.