Article Text

Abstract
An 81-year-old woman with a background of metastatic melanoma on pembrolizumab with no history of diabetes was brought into the emergency department with polyuria, polydipsia and weight loss. The initial assessment was consistent with severe diabetic ketoacidosis (DKA) and prerenal acute kidney injury with no clinical evidence of infection. The patient was treated with fluid resuscitation and an insulin infusion and eventually transitioned to a basal-bolus insulin regime, which was continued after discharge. Diabetes autoantibody screen returned negative, and she was diagnosed with immune checkpoint inhibitor–induced diabetes mellitus (ICI-induced DM) due to pembrolizumab. The patient has clinically improved and pembrolizumab was continued. The aim of this report is to highlight the importance of recognising ICI-induced DM as a rare immune-related adverse event in patients receiving programmed cell death protein 1/programmed cell death protein-ligand 1 inhibitor therapy and provide clinicians with insight into immune checkpoint endocrinopathies with an emphasis on diabetes and DKA.
- diabetes
- immunology
- skin cancer
- unwanted effects / adverse reactions
- acute renal failure
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
The use of immune checkpoint inhibitors (ICIs) is becoming increasingly prevalent in the management of solid tumours. Examples of ICIs include monoclonal antibodies that act on cytotoxic T-lymphocyte antigen-4 (eg, ipilimumab), programmed cell death protein 1 (PD-1) (eg, pembrolizumab, nivolumab) or programmed cell death protein-ligand 1 (PD-L1) (eg, atezolizumab, durvalumab, avelumab) and disinhibit antitumour immune responses. However, as these pathways usually function to provide immune self-tolerance, their usage can also lead to immune-related adverse events (irAEs) in various organ systems.1 2 Thyroid dysfunction and hypophysitis are more commonly reported immune-related endocrinopathies; however, immune checkpoint inhibitor–induced diabetes mellitus (ICI-induced DM) has also become recognised as a rarer adverse event with PD-1 or PD-L1 inhibitors.3 4 Significantly, the first presentation of patients with ICI-induced DM can be diabetic ketoacidosis (DKA), and we hope to add to the emerging literature around this condition.1 5–8
In this report, we describe the case of a patient with metastatic melanoma who developed severe DKA and ICI-induced DM secondary to pembrolizumab.
Case presentation
An 81-year-old woman presented to the emergency department of a regional hospital with a 24-hour history of nausea, vomiting and diarrhoea, and a week-long history of worsening polyuria, polydipsia and weight loss.
She had initially been diagnosed with malignant melanoma in her right heel 11 years prior, which was managed with resection. The melanoma recurred after 8 years and, despite multiple re-excisions during the intervening years, was found to have metastasised to her right knee around 6 months prior to her current presentation. The melanoma was BRAF and NRAS (neuroblastoma RAS viral oncogene homologue) negative and KIT positive. Her baseline endocrine workup prior to the start of pembrolizumab, which included blood glucose level (BGL), thyroid function tests (TFTs) and hypothalamic-pituitary-adrenal axis biochemistry, was all unremarkable. She was given a 3-weekly treatment regimen of pembrolizumab 2 mg/kg and had received eight doses prior to her presentation. The last dose was 2 weeks prior.
Her other medical history included atrial fibrillation, hypertension and left breast carcinoma that was managed with mastectomy and axillary clearance 15 years prior. Her medications were apixaban, metoprolol, lercanidipine and olmesartan/hydrochlorothiazide. She had no personal or family history of diabetes or other autoimmune conditions.
On examination, she appeared unwell and her Glasgow Coma Scale was 13 (E3, V4, M6); however, she was oriented to time, place and person. She was afebrile, her heart rate was irregular at 110–150 beats per minute, blood pressure was 110/78 mm Hg, respiratory rate was 24 breaths per minute and oxygen saturations were 100% on room air. She had an ejection systolic murmur, mild suprapubic tenderness on palpation and mild pitting oedema on her mid-shins.
Investigations
Bedside investigations showed a BGL >39 mmol/L (>702 mg/dL), ketones 7.6 mmol/L, lactate 6.65 mmol/L and metabolic acidosis with venous blood gas pH 7.05, HCO3 7.2 mmol/L, pCO2 25.9 mm Hg. Her urinalysis was positive for glucose (500 mg/dL), ketones (40 mg/dL) and protein (30 mg/dL). Her formal laboratory investigations are summarised in table 1. She had a high anion gap (35 mmol/L; reference 4–13 mmol/L), mildly elevated lipase and an acute kidney injury. Baseline renal function test results were as follows: creatinine 68 μmol/L and estimated glomerular filtration rate (eGFR) 72 mL/min/1.73 m2.
Laboratory results on day 1 of admission
A septic screen, which included urine and blood cultures and a chest X-ray, did not demonstrate any signs of infection.
Based on these findings, she was diagnosed with DKA. The underlying cause was considered to be ICI-induced insulin-dependent diabetes mellitus. Islet autoantibodies (anti-glutamic acid decarboxylase (anti-GAD), Islet antigen-2 and zinc transporter 8, TFTs and adrenocorticotropic hormone/cortisol were also ordered.
Treatment
The patient was managed according to DKA guidelines, and her repeat ketones and venous blood gas results were much improved. Following discussion with the intensive care unit at the tertiary referral centre, the patient was admitted to the regional hospital under the care of the general medicine/endocrinology team. After the insulin infusion was ceased, the patient was transitioned to a basal-bolus insulin regime. Her acute kidney injury resolved, and her endocrinopathy and autoantibody screen returned negative (table 2). She was discharged with a plan for follow-up with an endocrinologist, a dietician and a diabetic educator.
Endocrine laboratory results
Outcome and follow-up
The patient resumed pembrolizumab treatment after discharge from the hospital due to the positive clinical response for her melanoma. Her diabetes was followed up in the endocrinology outpatient clinic, where her glycaemic control was found to be improving but still suboptimal, with an haemoglobin A1C (HbA1c) of 8.9% and fasting BGL of 7.9 mmol/L. Her insulin regime also required ongoing titration as she began experiencing intermittent hypoglycaemic episodes. Later, metformin was also initiated as an adjuvant therapy to insulin. Additional hormone testing was performed to exclude other ICI-induced endocrinopathies (thyroid or pituitary dysfunction) and the results were all within normal reference ranges (table 3). She also underwent a dexamethasone suppression test which was normal.
Endocrine laboratory results
Discussion
Pembrolizumab is an IgG4 monoclonal antibody that is licensed for treatment of melanoma and various solid malignancies, including non-small cell lung carcinoma, head and neck squamous cell carcinoma, classical Hodgkin lymphoma, primary mediastinal B-cell lymphoma and urothelial carcinoma.
The PD-1 pathway promotes tolerance to self-antigens and prevents damage to normal tissues during an immune response. PD-1 is expressed on T cells and PD-L1 is expressed on tumour cells and macrophages. When PD-L1 binds to PD-1, the T cells are deactivated; therefore blockade of PD-1 or PD-L1 prevents this deactivation and promotes tumour destruction.9
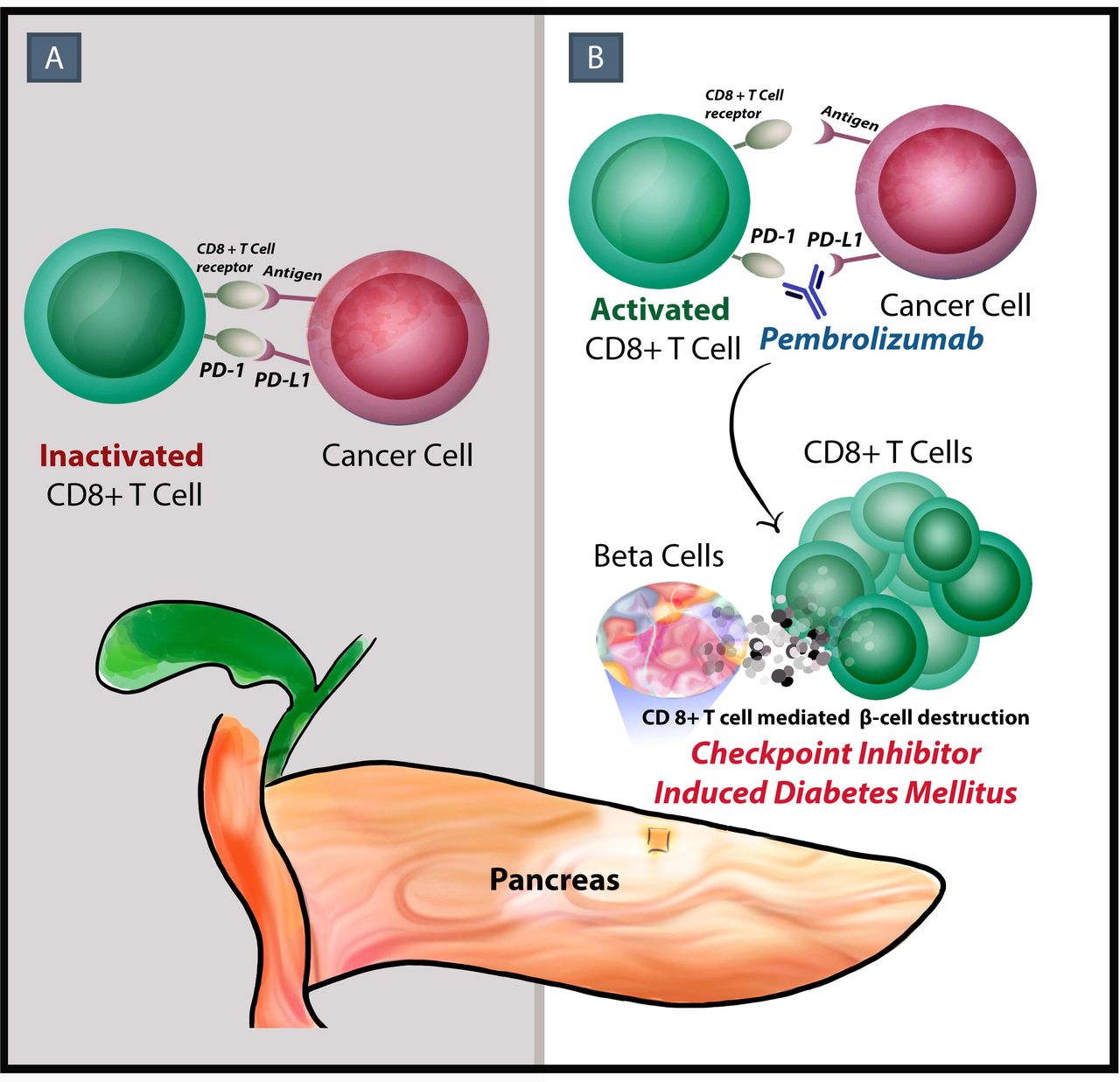
The mechanism of PD-1 and PD-L1 associated or ICI-induced DM is not well understood.10 11 It has been suggested that the PD-1 pathway may be inhibitory in the development of type 1 diabetes mellitus (T1DM); in preclinical studies, it has been shown that PD-L1 is expressed on the islet cells of non-obese diabetic (NOD) mice and PD-1 and PD-L1 blockade precipitates diabetes by interrupting this immunoregulatory process.8 11–16 It has also been demonstrated that patients with autoimmune diabetes have a significant reduction in PD-1 expression on helper T cells (CD4 T cells), which may result in abnormal activation of cytotoxic T cells (CD8 T cells) and the destruction of beta cells (figure 1).17 18

{kind=link}
(A) Programmed cell death protein-ligand 1 (expressed by tumour cells) binds to programmed cell death protein 1 (PD-1) and T cells are deactivated. (B) Pembrolizumab (anti PD-1 monoclonal antibody) can rarely cause an abnormal cytotoxic T cell (CD8+ T cell) mediated beta cell destruction and development of immune checkpoint inhibitor–induced diabetes mellitus (ICI-induced DM). Illustrated by Dr Ahmed Almuwais.
There is some discrepancy in the literature regarding the classification of ICI-induced diabetes as T1DM or fulminant T1DM (FT1DM), and it has been suggested that ICI-induced DM is a distinct pathophysiologic entity with features of both.11 19–22
The characteristic features of ICI-induced DM are described as acute onset of hyperglycaemia, higher frequency of ketosis, rapid decline in C-peptide concentrations and high glycaemic variability in keeping with the absence of residual beta cell function.5 6 11 22 23
The time from initiation of ICI to development of ICI-induced DM is variable, ranging from weeks to more than a year after initiation of therapy, with a case series by Galligan et al indicating the majority of patients present within the first month.4 6 11 19 21 22 24
T1DM is characterised by absolute insulin deficiency secondary to T cell–mediated beta cell destruction and beta cell–associated serum autoantibodies.25 26 FT1DM, which has generally been reported in East-Asian populations, is characterised by extremely acute onset of hyperglycaemia, ketoacidosis, near-normal HbA1c, elevated levels of pancreatic enzymes, severe insulin deficiency and negative autoantibodies.4 20 21 27 28 In addition to the mixed characteristics noted above, the older age at diagnosis (range 22–84 years), rapid presentation to insulin deficiency and absence of a ‘honeymood period’ is seen to differentiate ICI-induced DM from T1DM, and the sudden loss of beta cell function is thought to differentiate it from latent autoimmune diabetes in adults.1 6 10 11 19 29 Pancreatic enzymes are noted to be elevated in approximately half the cases of ICI-induced DM; however, this may be related to the non-specific elevations that occur in 16%–25% of cases with DKA, and has also been reported to occur in the absence of new onset diabetes in patients receiving ICIs.1 5
There is also variability in the literature as to whether ICI-induced DM is associated with islet autoantibodies.6 23 Some studies suggest the majority of patients are autoantibody negative when compared with those with T1DM, whereas others indicate at least one islet autoantibody (most commonly anti-GAD) is present in 30%–50% of cases.4–7 11 22 23 It has also been noted that patients with positive anti-GAD had a shorter time from PD-1 inhibitor initiation to the onset of ICI-induced DM.4–7 30 31
The variability in autoantibody status further indicates the poorly understood nature of the mechanism of ICI-induced DM.32 33 Similarly, the NOD mouse model indicated there was no correlation between autoantibody levels and the development of autoimmune diabetes in subjects receiving PD-1/PD-L1 inhibitors.12 Some authors suggest that PD-1 inhibitor therapy may trigger sudden and major activation of beta cell reactive T cells, without involvement of humoral immunity prior to presentation with overt diabetes, and this could account for the autoantibody negative status of some patients.20 Additionally, it is unclear if the autoantibodies are present prior to initiation of ICIs or are developed after, so the usefulness of autoantibodies to predict individuals at risk of ICI-induced DM remains unknown.1 7 30 34 35
A number of factors have been identified which are thought to increase a patient’s risk of developing ICI-induced DM, including personal or family history of autoimmune conditions, and the presence of another irAE, most commonly thyroiditis.1 4–6 11 36 Patients on a combination of immunotherapies, or with a history of treatment with other immunotherapies, also appear to be at an increased risk.8 32 33 36 37
Certain human leukocyte antigen (HLA) class II haplotypes have been associated with FT1DM (DRB1*04:05-DQB1*04:01 and DRB1*09:01-DQB1*03:03) and T1DM (DRB1*04:01-DQB1*03:02 or DRB1*03-DQB1*02).10 28 38 39 Some case reports suggest an association with T1DM high-risk class II haplotypes in ICI-induced DM, but others have indicated no association or ICI-induced DM occurring in patients with ‘protective’ haplotypes (respectively, DRB1*15:01-DQB1*06:02, DRB1*11:01-DQB1*03:01 and DRB1*13-DQB1*06).4 20 23 36 39–41 Given the variability in the literature, further research is required to determine the clinical utility of autoantibody screening and HLA typing in predicting the development of ICI-induced DM.7 9 19 39
Cases of ICI-induced DM have been increasingly reported since 2015; however, the exact incidence is unknown.8 40 42 The reported incidence of ICI-induced DM has ranged from 0.9% to 1.9%, and one meta-analysis of ICI clinical trials indicated a 0.2% frequency of patients developing FT1DM and another reported a frequency of 1%.1 4 11 37 Given the hypothesised pathophysiology of ICI-induced DM, it remains unclear as to why the proportion of patients who develop ICI-induced DM is comparatively low.11
Further research into this condition and its pathophysiology is required to facilitate refinement to the current guidelines and assist in development of risk stratification tools and monitoring protocols.1 10 19 Clinicians should be sensitised to the risk of abrupt onset hyperglycaemia and DKA.10 22 41 43
In terms of management of ICI-induced DM, the majority of the reported cases, including our own, involve acute management for DKA following standard protocol, and subsequent management as for T1DM.19 Other irAEs are frequently managed with immunosuppressive doses of corticosteroids; however, this has not been found to be effective in reversing islet cell destruction in ICI-induced DM and patients subsequently suffer from permanent insulin deficiency.1 5 7 20 22 23 34
The American Society of Clinical Oncology guidelines recommend withholding ICIs until glucose control is achieved, unless the patient has no evidence of ketosis or serologic evidence of T1DM, in which case the ICI may be continued in addition to initiating diabetes management.44 Current literature generally supports resumption of the ICI, especially in the setting of a positive anti-tumour response.4 5 10 11 19 44 45
Due to the high risk of morbidity and mortality from severe DKA, and the long-term morbidity of T1DM, it is important for physicians and patients to be aware of this complication of ICIs.4 6 8 10 The European Society for Medical Oncology recommends monitoring of blood glucose in patients receiving ICIs.3 The American Society of Clinical Oncology guidelines recommend measuring BGL at baseline and with every treatment cycle for 12 weeks, then ongoing every 3–6 weeks.44 The Japanese Diabetes Society recommends measuring BGL at every visit involving drug administration and consultation with an endocrinologist for a definitive diagnosis of diabetes if a patient has hyperglycaemic symptoms or hyperglycaemia.21
Assessing HbA1c prior to initiation of ICIs, and self-monitoring of BGLs have also been suggested as ways to identify initial elevations in blood glucose.1 6 7 However, a study by Magis et al found that monitoring of glycaemia in patients receiving PD-1 inhibitors was ineffective in anticipating the acute onset of DKA in ICI-induced DM.41 It has also been suggested that patients with T2DM should have autoantibody levels done prior to initiation of ICIs for risk stratification, given the risk that new ICI-induced DM may be mistaken for uncontrolled T2DM.42
Patient education around the symptoms of hyperglycaemia and DKA may be a more effective measure for earlier case identification.7 10 24 41 43 46 Notably, our patient had unremarkable BGLs on routine monitoring bloods during her pembrolizumab treatment, but reported a week-long history of polyuria and polydipsia prior to presenting in acute DKA.
In conclusion, ICI-induced diabetes is a rare but significant complication of ICIs, and as with other endocrinopathies, tends to be irreversible.47 With the increasing use of checkpoint inhibitors in cancer management and implementation of combination therapy, the incidence of this complication is likely to increase.5 22 Discussion around the risk of irAEs should be routine in consent procedures, and patients receiving anti-PD1 therapy should receive education around symptoms and signs of hyperglycaemia and ketoacidosis to promote earlier presentation and diagnosis. Further investigation and research into the pathophysiology of this condition is required to facilitate identification of potential screening tests for patients at greater risk of developing ICI-induced DM as well as to guide management or preventative strategies for this complication.
Learning points
Immune checkpoint inhibitor–induced diabetes mellitus is a rare but clinically important immune-related adverse event (irAE) of programmed cell death protein 1 (PD-1)/programmed cell death protein-ligand 1 (PD-L1) inhibitors as it does not appear to undergo remission and diabetic ketoacidosis is often the first presentation
Healthcare professionals should be aware of this irAE, and patients receiving PD-1/PD-L1 inhibitor therapy should receive education around symptoms of hyperglycaemia and ketoacidosis to prompt early presentation and case identification
Further research is required to determine the applicability of islet autoantibody, human leukocyte antigen or C-peptide screening as a way to risk stratify patients
Ethics statements
Patient consent for publication
References
Footnotes
Contributors Supervised by AZI. Patient was under the care of AZI. Report was written by AZI, AA and HG.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.