Article Text

Statistics from Altmetric.com
Description
A 27-year-old woman was referred to the pulmonary office for evaluation of incidentally identified radiologic chest abnormalities. The patient was recently seen in her primary care provider’s (PCP) office twice in the past 6 weeks for low grade fever, cough, chest pain and shortness of breath. She was diagnosed with acute bronchitis and treated with antibiotics with subsequent resolution of her symptoms. As a part of her workup, she underwent imaging studies which prompted the office visit.
The patient was an active smoker with a 15-pack year history of smoking and currently smoked a pack a day. In the office, she denied any cough, sputum production, wheezing, hemoptysis or shortness of breath. She had no known medical condition and was not on any home medication. She appeared comfortable. Her vital signs were within normal range. The physical examination was entirely normal. No abnormalities were present on the chest examination, including auscultation.
A chest X-ray obtained 2 weeks ago by the PCP was also normal (figure 1). A computed tomographic angiogram (CTA) of the chest revealed no pulmonary embolism. However, distinct areas of hyperlucency and hyperinflation involving the anterior segment of the right upper lobe (RUL) and medial segment of the right middle lobe (RML) were seen (figure 2). A mucus filled, dilated, branching tubular structure was present in the RUL without any identifiable communication to the proximal central airways (figure 3). Additionally, a hypoplastic airway leading to the medial segment of the RML without mucus plugging was also seen (figure 4). The radiologic features were consistent with congenital bronchial atresia (CBA) of the anterior segment of the RUL and congenital segmental emphysema syndrome (CSES) of the medial segment of the RML.

Posteroanterior chest X-ray revealed no pulmonary infiltrates.
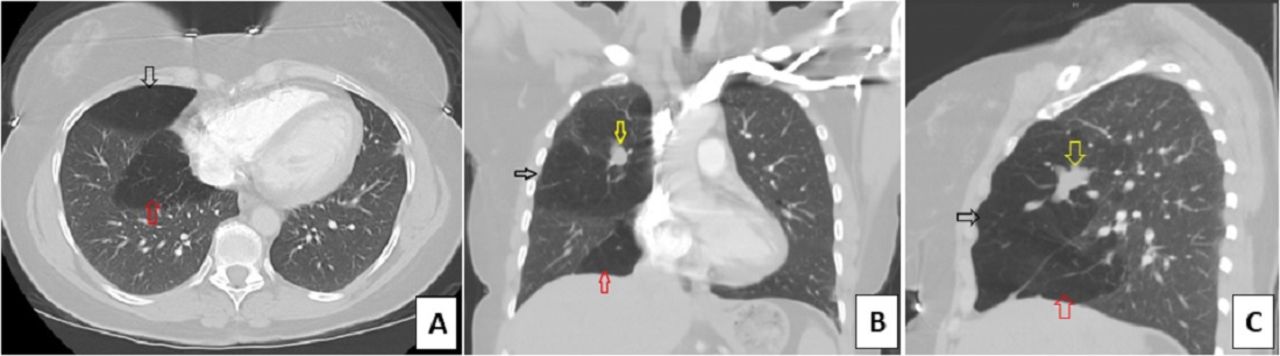
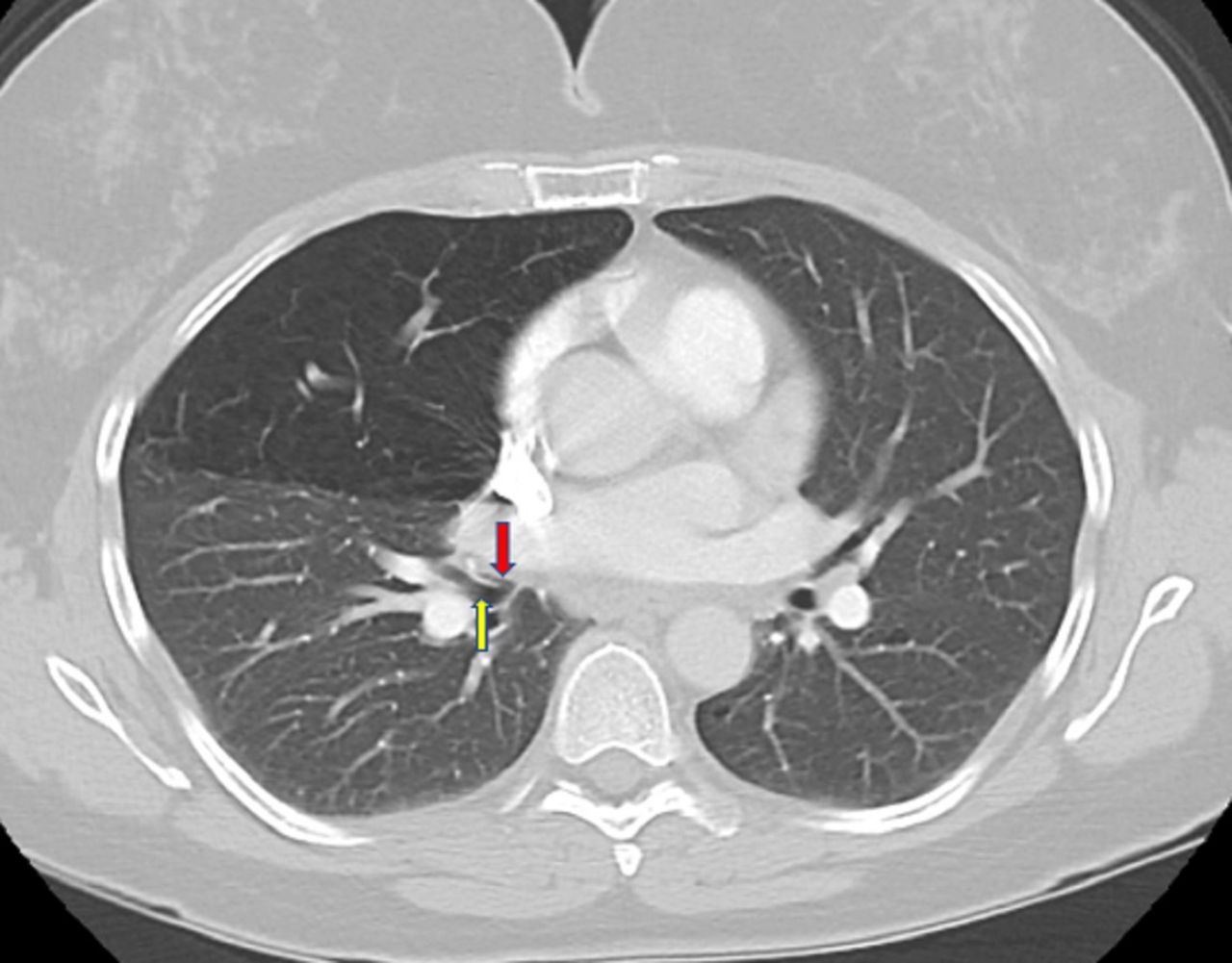
CT of the chest in axial (A), coronal (B) and sagittal (C) views demonstrating hyperlucent and hyperinflated anterior segment of right upper lobe (RUL) (black arrow) and medial segment of the right middle lobe (RML) (red arrow). Blind, dilated and mucus filled bronchocele (yellow arrow) was present in the RUL.
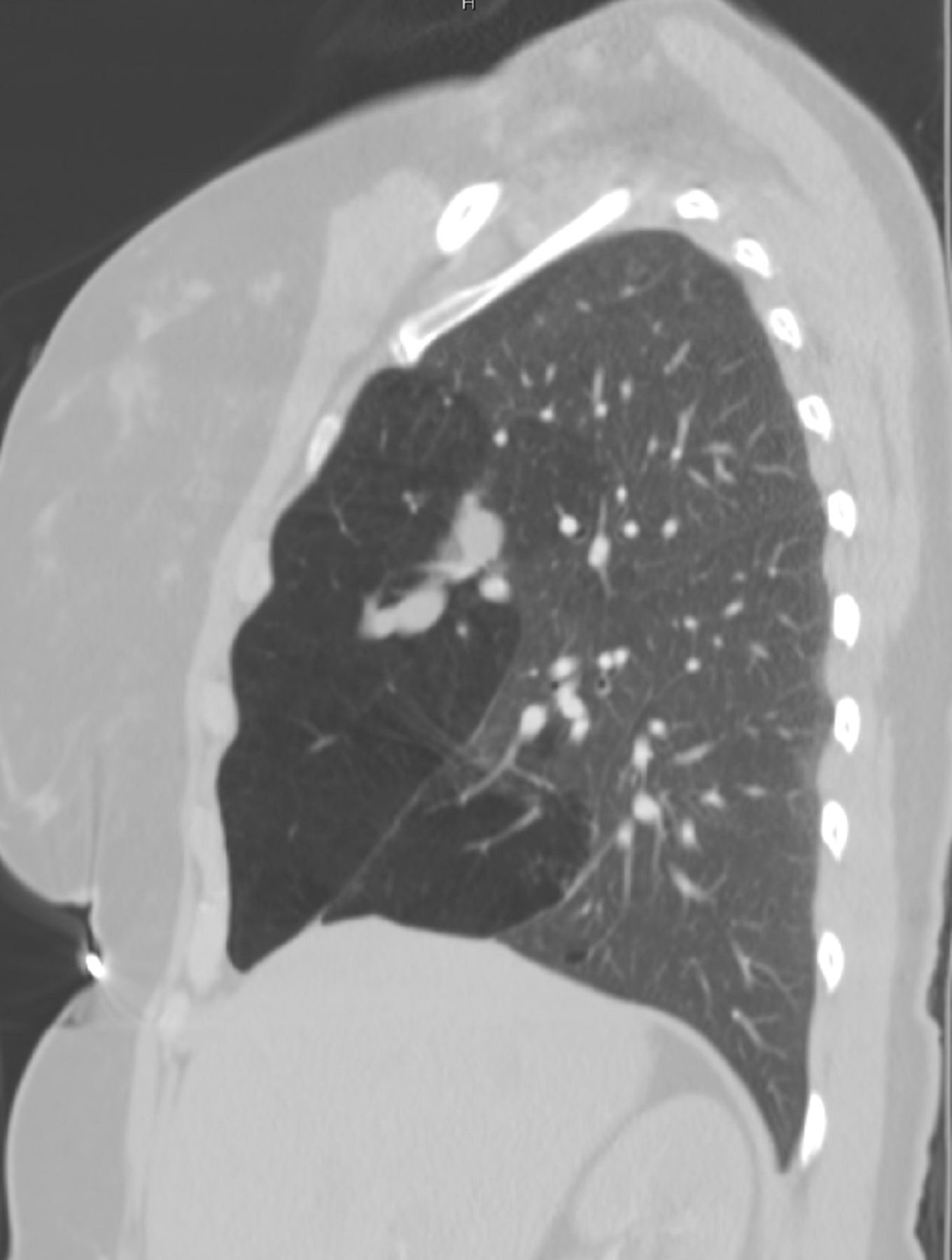
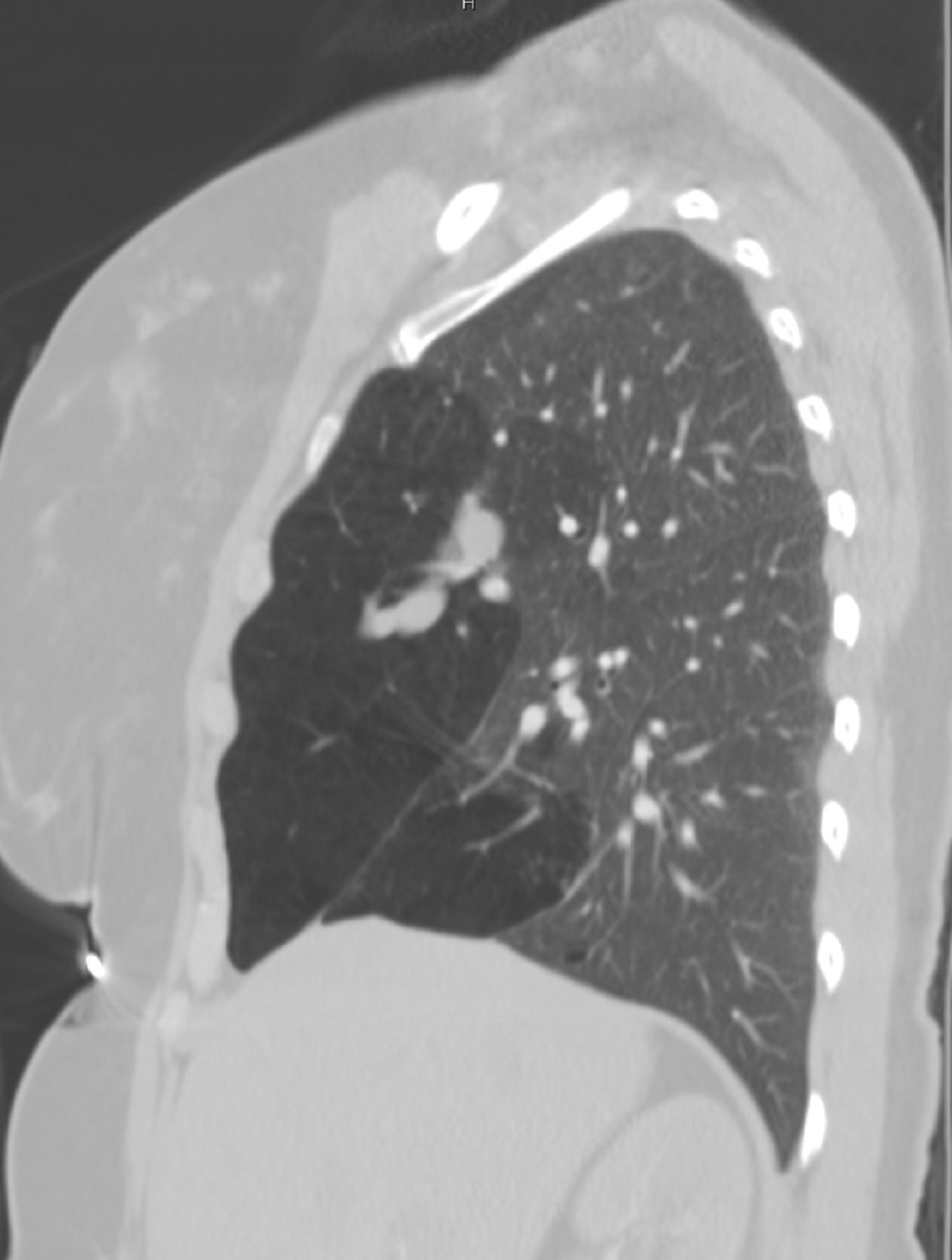
Sagittal CT scan view showing hyperlucent anterior segment of right upper lobe (RUL) with a tubular branching structure. The hyperlucent and hyperinflated medial segment of the right middle lobe (RML) was also visualised.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
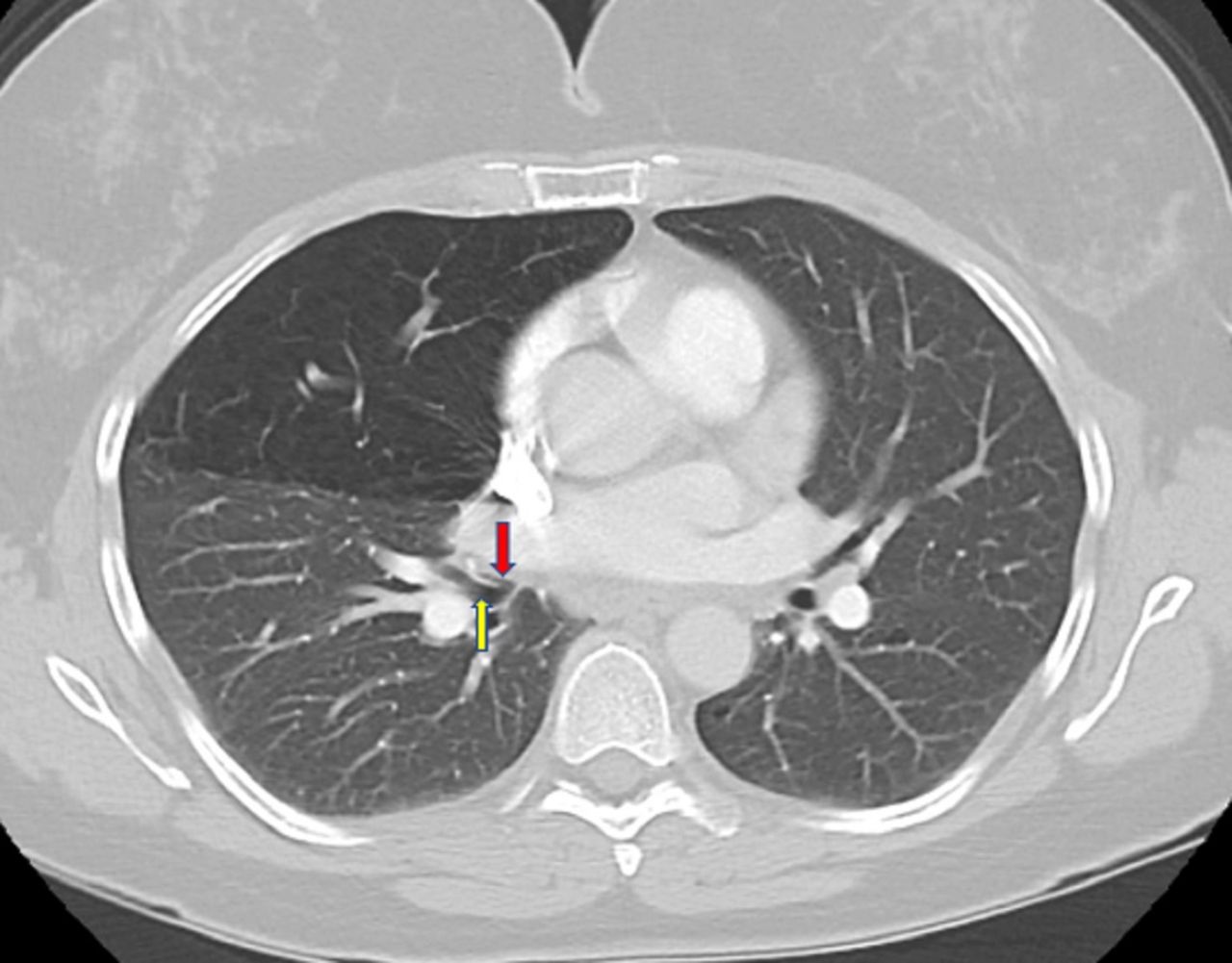
Axial CT scan showing atretic and narrow airway leading to the medial segment of right middle lobe (RML) (red arrow). The lateral segment bronchus is significantly wider in comparison (yellow arrow).
Adult congenital pulmonary anomalies (CPAs) are rare entities. Therefore, a stepwise clinical and radiologic evaluation is necessary for appropriate diagnosis and management of these patients. CPAs can be further differentiated into pulmonary parenchymal anomalies (PPA), vascular anomalies or a combination of the two. Clinically encountered PPA in adult patients include CBA, CSES and congenital lobar emphysema (CLE). Bronchopulmonary sequestration (BPS) represents a combined parenchymal and vascular malformation. Although technically not a CPA, but Swyer-James-Macleod syndrome (SJMS) is an important radiologic differential in these patients. The presence of more than one anomaly in an adult patient is infrequently described in the literature. Our patient suffered from both CBA and CSES.
CBA is anatomically characterised by a proximally blind, mucus filled, dilated airway that lacks anatomic connection to the hilar structure, known as bronchocele, with localised hyperinflation of the lung.1 The bronchocele develops due to a traumatic or vascular event during the intrauterine life. The bronchial tree follows a sequential growth pattern post conception. The development of the lobar bronchus starts during the fifth intrauterine week, and the distal airways are completed by week 16.2 In CBA, the airways distal to the atretic airway are normal with functioning goblet cells that are responsible for mucus accumulation. Since the smaller airways develop normally, the vascular insult likely occurs after 16 weeks of gestation. In some patients, a fibrotic band may connect the bronchocele to the proximal airways.3
CBA is more prevalent in men than women. It commonly affects the segmental bronchus, but lobar or subsegmental airways can also be involved. The left upper lobe (LUL) is the most frequent location.4 The affected segment receives air by collateral ventilation through the pores of Kohn and channel of Lambert, because the airway is nonfunctional and unable to deflate. This results in progressive hyperinflation, raising the possibility of compression of the adjacent healthy lung.5 Most patients with CBA are asymptomatic and diagnosed incidentally on imaging studies. However, a minority of patients suffer from infectious complications requiring antibiotic therapy. In rare cases, surgical removal of the affected segment may be necessary.3
Although previously considered a part of the CLE spectrum, CSES appears to be a distinct entity.6 The pathophysiologic basis for the development of CSES is different from CLE. In fact, there are more similarities between CBA and CSES than CLE. In patients with CSES, the segmental bronchus is nonfunctional, ectatic and could be mucus impacted. However, there is no anatomic discontinuity between the segmental bronchus and hilar structures, and there is no bronchocele. CSES also follows a predictable course of evolution. Due to the lack of airflow through the diseased bronchus, the affected segment appears solid at birth, with areas of hyperlucency.7 Over time, the segment receives collateral ventilation and becomes hyperlucent and hyperinflated. The alveolar tissue of the affected segment is completely differentiated with intact pulmonary circulation. Histopathologic analysis of the affected segment reveals hyperinflated rather than cystic lung tissue.
In contrast, CLE has a functional airway leading to the affected lung lobe, or rarely, a lung segment.8 The pathobiology of CLE involves the creation of a one-way ‘ball valve’ mechanism that allows inspiratory airflow but prevents the expulsion of the air during exhalation causing gradual air trapping and hyperinflation.9 This unidirectional airflow could result from either an extrinsic or intrinsic obstruction. An extrinsic obstruction can be caused by anomalous pulmonary vascular return or a vascular sling. Intrinsic obstruction, which is more commonly seen, can result from a mucosal fold, absent cartilage, mucus plug or airway granuloma.9 Due to progressive lobar expansion, most patients become symptomatic early in life. The lung hyperinflation may cause compression and atelectasis of the ipsilateral or contralateral lungs and mediastinal shift. Similar to CBA, the LUL is affected most frequently. Lung histopathology demonstrates alveolar overdistention without definitive damage.10 The incidence of CLE is higher in males and patients typically present in the neonatal period.11 However, adults can present with CLE if the degree of hyperinflation is modest.12–14 Another CPA that could be confused with CBA is BPS. Additionally, SJMS may have a similar radiologic appearance.
Swyer-James syndrome or SJMS is a complication of recurrent pulmonary infection during childhood. The infectious agents could be bacterial, viral or mycobacterial. Commonly implicated pathogens include Mycoplasma pneumoniae, Bordetella pertussis, Influenza A, Paramyxovirus, Adenovirus and Mycobacterium tuberculosis.15 The infection results in progressive destruction of the airways distal to the fourth or fifth generation bronchus causing obliterative bronchiolitis and bronchiectatic club-like airways. Patients typically present with hyperlucent hemithorax on chest radiology. The affected lung demonstrates normal or smaller lung volume.16 One striking feature of SJMS is a profound diminution of pulmonary artery calibre and circulation to the affected lung.17 The CT angiogram or ventilation-perfusion scanning in patients with SJMS can be confused with unilateral absence of pulmonary artery (UAPA). Cases of UAPA are often associated with cardiac malformation. In isolated UAPA, there is increased systemic collateral circulation of the affected lung through the bronchial, intercostal, supra and subdiaphragmatic aortic branches.18 Pulmonary oligemia is present on chest radiology, but typical features of SJMS, as described above, are absent.
BPS describes the presence of lung tissue within the normal lung parenchyma that has two distinctive features: (1) They do not communicate with the tracheobronchial tree and (2) they receive their blood supply from the aorta.19 BPS is an anomaly of the lower airway and develops early in the developmental process. BPS could be intralobar, extralobar or associated with congenital adenomatoid malformation. On CT chest, BPS appears as a solid mass that could have cystic changes. Identification of systemic arterial supply on CTA is diagnostic of BPS.20 The left lower lobe is the most commonly affected site.
The treatment for CPAs in adult patients depends on the severity of symptoms, anatomic progression of the disease and the degree of pulmonary function impairment. For example, an incidentally identified CPA that is not symptomatic could be managed conservatively. On the other hand, patients with severe symptoms such as recurrent chest infection, or progressive hyperinflation of the affected lung causing compression of the adjacent healthy pulmonary parenchyma leading to impaired pulmonary function and shortness of breath, may benefit from surgical resection of the anomalous tissue.
Learning points
Congenital bronchial atresia (CBA) is a rare disease characterised by the formation of a proximally blind mucus filled atretic airway (bronchocele) and localised lung hyperinflation.
Congenital lobar emphysema, congenital segmental emphysema syndrome and Swyer-James syndrome can all present with lung hyperinflation, but the pathophysiologic mechanism of each is different from CBA.
Simultaneous presence of two congenital pulmonary anomalies (CPAs) is infrequent in adults but need to be kept in mind. If associated with respiratory impairment, CPAs may require definitive surgical intervention.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors SS, AA and AB planned the study and collected data. SS, AA, AB and BKS prepared the initial manuscript. All authors finalised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.