Article Text

Abstract
Parathyroid cysts (PCs) are rare benign lesions representing between the 0.08% and the 0.34% of the neck masses going on surgery. They should be considered in the differential diagnosis of neck masses, especially in the differential diagnosis of the cystic anterior neck masses.
Approximately 300 cases of PC are reported within the international literature.
The gold standard for diagnosis is the evidence of high-level intact parathyroid hormone in cystic fluid. It is important to diagnose PCs before surgery, not intraoperatively, in order to avoid unnecessary surgeries or superfluous excision of part of the thyroid gland and prevent the patient from iatrogenic hypothyroidism.
A surgical approach is required in those patients with large-sized cysts, relapses despite needle aspirations or if it causes hyperparathyroidism.
We describe a case report of a patient, initially misdiagnosed with a thyroid cyst swelling, who instead had a giant non-functioning PC, which produced dyspnoea or dysphagia.
- Endocrine system
- Head and neck surgery
- Ultrasonography
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
This is a case of misdiagnosed parathyroid cyst (PC). Because of the higher prevalence of the thyroid cysts, PCs can be misunderstood,1 2 delaying the proper treatment or missing the right surgical approach.
Case presentation
A woman in her 40s was referred to our endocrine surgery unit with a 10-year history of lump in the right side of the neck. She reported significant compressive symptoms, such as dysphagia for liquid and solid food, and a mild restrictive respiratory failure due to tracheal compression.
The cystic lesion was initially misdiagnosed for a thyroid cyst and was treated with several fine needle aspiration (FNA) during the years, but it always relapsed after a few months.
Investigations
Conventional ultrasound reported a 57×37×42 mm cystic lesion in the inferior right lobe of the thyroid (figure 1). The fluid aspirated was a clear water fluid, and when the level of intact parathyroid hormone (iPTH) in cystic fluid liquid was evaluated, it revealed that the cyst arose from the parathyroid (cystic iPTH dosage: 151.8 pg/mL).

Ultrasound imaging.
Just about 10% of the PCs are associated with hyperparathyroidism; thus, it is important to perform laboratory tests to exclude a functioning one. In our case, the parathyroid function value showed normal level of calcium (9.6 mg/dL) and PTH (51.8 pg/mL) in the blood.
A preoperative CT scan highlighted the neck mass surrounding and displacing the trachea on the left with no evidence of local invasion (figure 2).

Preoperative CT scan showing the neck mass surrounding and displacing the trachea: (A) coronal scanning; (B) axial scanning; (C) sagittal scanning.
Differential diagnosis
The presentation of PCs is very similar to thyroid cysts, which are much more prevalent pathologies of the anterior neck. The only way to make a correct diagnostic and therapeutic evaluation is to take into account the existence of the PCs, and plan the proper diagnostic work-up.3 4
During evaluation of a neck mass in the central region, ultrasound is the first-level diagnostic test. As an alternative, CT and magnetic nuclear resonance can also show a neck mass with cystic content. In all cases, imaging tests are indicative of cystic neck lesion but are inconclusive.
Second, if the ultrasound finds out a cystic mass, it is recommended that a cytological examination of both the fluid and the dosage of the PTH level in the fluid is performed. The FNA procedure is therapeutic and diagnostic at the same time: it allows to evacuate and reduce cystic volume and to perform PTH dosage in the cystic fluid.
Treatment
Considering the numerous relapse episodes, we decide, according to the patient, to refer her to surgery.
In the operating room, before skin incision, we performed an ultrasound-guided suction procedure of 60 mL of a clear colour cystic fluid, obtaining a mild but temporary reduction of the volume of the cyst, in order to perform a minimally invasive cervicotomy.
The cystic formation was found in the inferior portion of the thyroid lodge and the isthmus and the superior part of the mediastinum.
The thin-walled cyst had developed adherence on the pre-thyroid muscles, on the inferior and the medium part of the right thyroid lobe, on the isthmus and on the right thyrothymic ligament.
Surgery went on accurate dissection, separating the cyst from the adherence with muscles and thyroid gland, until the mediastinum and from the thyrothymic ligament.
The inferior laryngeal nerve was well identified at the origin in the mediastinum; additionally, the inferior parathyroid gland was identified in its typical place and appeared normal in size and morphology. The cyst was completely removed, preserving thyroid gland integrity carefully. A final check of the surgical field was good, and no drainage was needed. The minimally invasive incision was closed with an absorbable suture.
Outcome and follow-up
No complications occurred postoperatively. The patient was discharged on day 2 and went back to work in a week. A final anatomical pathology report confirmed a PC with typical parathyroid cells (‘chief cells’) (figures 3–6). The patient was really satisfied with the surgical outcome (figure 7).

Postoperative specimen.

The anterior cut of the surgical specimen showing the inner cavity of the cyst.
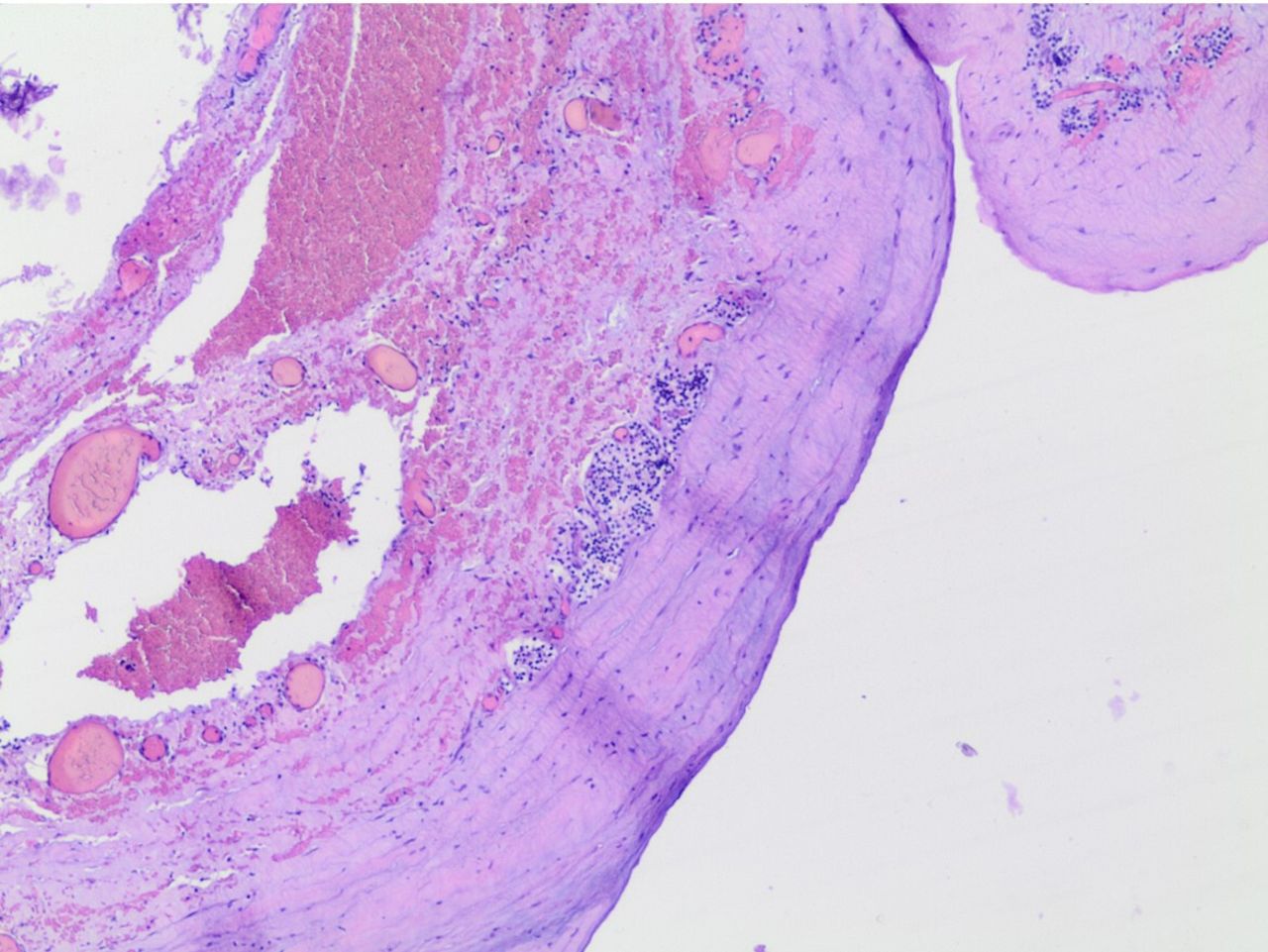
The wall of the cyst, formed by parathyroid cells, coloured with H&E.

Magnification of the previous image, showing the parathyroid cells (chief cells).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The scar 3 months after surgery.
The follow-up was planned with a periodical ultrasound imaging.
Discussion
PCs are rare benign lesions of the parathyroid glands that represent less than 0.5% of the parathyroid gland disorders, but they should be considered in the differential diagnosis of neck masses, especially in the differential diagnosis of the cystic anterior neck masses.5
The first case of PC was reported by Sandstrom6 in 1880, and the first surgical excision of a PC was made in 1905 by Goris.7
The masses of the anterior region of the neck can be solid or cystic; the differential diagnosis of cystic cervical masses includes thyroid cyst, thymic cyst, thyroglossal duct cyst, lateral branchial cyst, bronchogenic cyst and PC.3 4
There are two types of PCs, which depend on their ability to secrete hormones: functioning and non-functioning ones. The non-functioning ones are more frequent than the functioning ones. They can present with a wide variety of symptoms, from asymptomatic neck masses to the different clinical manifestations of hyperparathyroidism and can be found from the angle of the mandible until the mediastinum.8
Most studies support FNA as the gold standard to distinguish PCs; it shows elevated PTH in the clear water cystic fluid.9
The treatment depends on the clinical presentation: non-functioning PCs are first treated with FNA, and then surgically excised if they recurs, while functioning PCs are treated with surgical excision.3 8 Careful dissection is the key to successful management, in order to avoid the rupture of the thin wall of the cyst.3 8
In this case, the patient was at first treated for a simple thyroid cyst.
Because of the macroscopic characteristic of the fluid (bright and aqueous), we decided to measure the PTH in the cystic fluid, according to the main literature. The diagnosis was made before surgery. The patient was not subjected to unnecessary procedures and there were no hypothyroidism and hypoparathyroidism. Our diagnostic approach agreed with the other studies described in literature. As Silva et al explained in their paper,3 it is important to exclude PC during the evaluation of a patient with a neck cystic mass.
Learning points
Parathyroid cysts had to be considered in the differential diagnosis of the anterior cystic neck masses.
Diagnosis is made by the finding of high levels of parathyroid hormone in the cystic fluid.
Surgical treatment is reserved to ones with large size tending to relapse despite needle aspirations.
Ethics statements
Patient consent for publication
Footnotes
Contributors AD wrote and revised the article and is the guarantor. LL performed the literature search and wrote the first draft of the article. RB revised the article. CPL revised the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.