Article Text

Statistics from Altmetric.com
Description
Following surgical debridement for Fournier’s gangrene, a morbidly obese man (250 kg, Body Mass Index 87 kg/m2) was admitted to the intensive care unit (ICU) in septic shock and multiorgan failure. His medical history included type 2 diabetes mellitus, dyslipidaemia, gastro-oesophageal reflux disease and atrial fibrillation. The severity and chronic end organ dysfunction of his comorbidities was unknown as the patient avoided doctors due to embarrassment of his weight.
On arrival to ICU, he was anuric and a decision was made to insert a dialysis catheter and start continuous renal replacement therapy (CRRT). The procedure to place an ultrasound-guided dialysis catheter into the left internal jugular vein was uncomplicated, although a routine chest X-ray (figure 1) prior to starting CRRT raised concern for arterial placement.
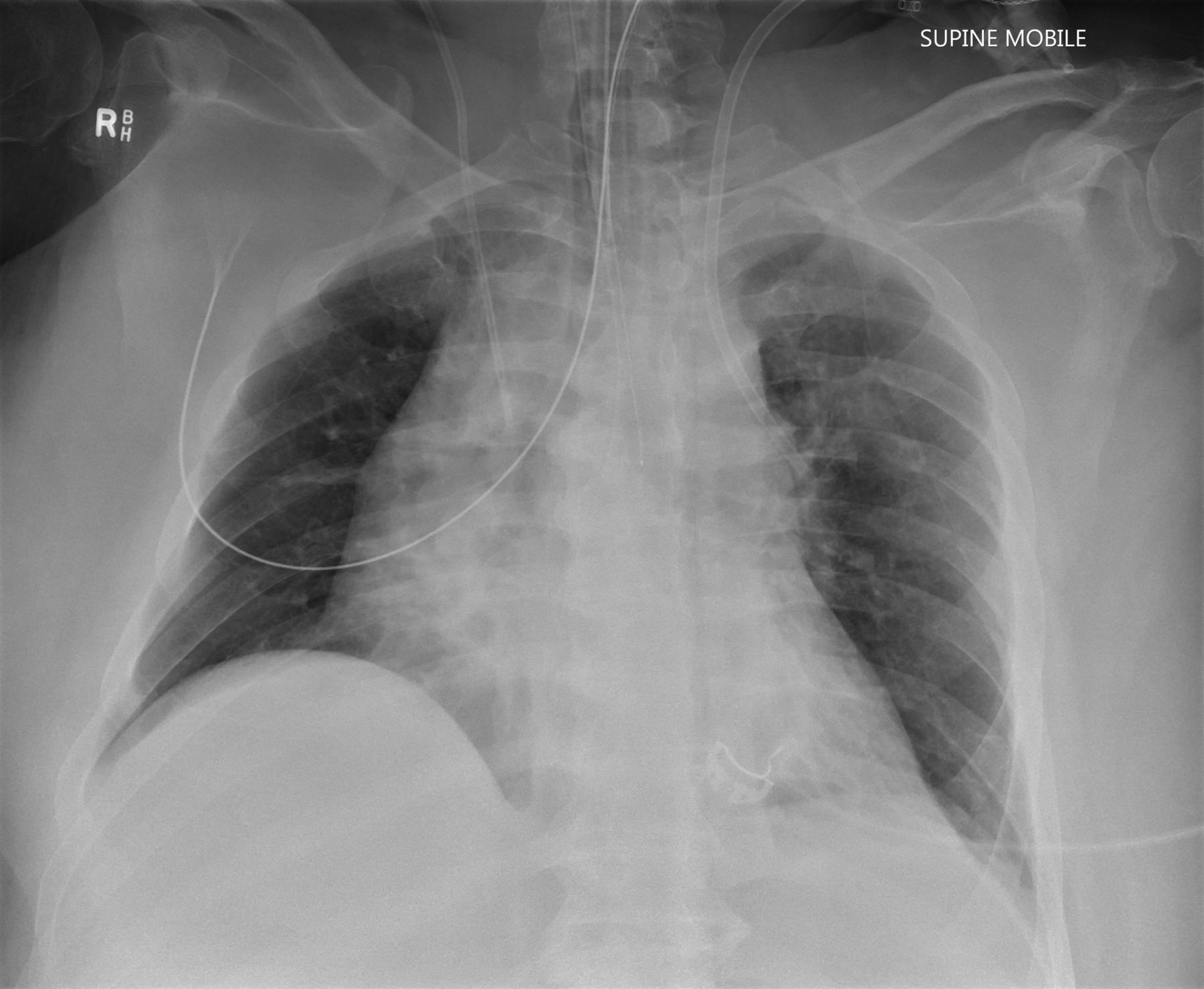
Chest X-ray with left-sided dialysis catheter and right-sided central venous catheter.
Transducing the pressure showed a pulsatile waveform with a pressure of 34/16 mm Hg (mean 22 mm Hg). The central venous pressure measured from a catheter in his right internal jugular vein was 18 mm Hg and an intra-arterial line blood pressure was 125/67 mm Hg. While the pressures ruled out arterial placement, concern for malposition still existed. Blood gas analysis, on FiO2 0.5–0.55, revealed oxygen partial pressures (PO2) 294 mm Hg from the dialysis catheter, 49 mm Hg from the central venous catheter and 68 mm Hg from the arterial line.
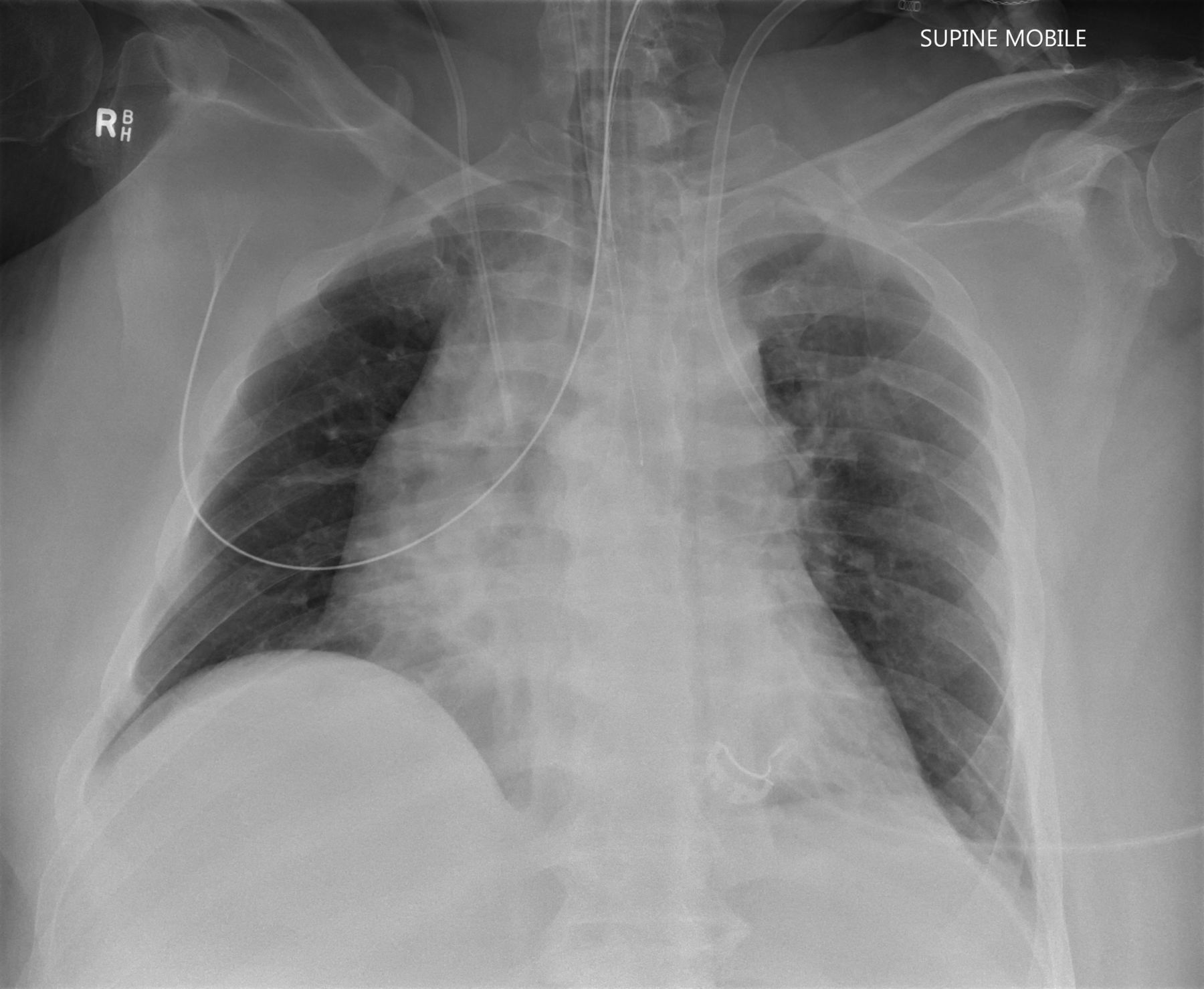
Given the striking differences in the PO2, catheter placement in an anomalous pulmonary vein seemed the only physiologically plausible explanation. Contrast CT scan confirmed the left upper lobe pulmonary vein drained into the brachiocephalic vein. The patient was transferred to interventional radiology (figure 2), and the catheter was redirected to the superior vena cava/right atrium junction under fluoroscopic guidance.

{kind=link}
{kind=link}
Contrast injected into the catheter illuminating the left upper lobe partial anomalous pulmonary venous connection.
With the advent of bedside ultrasound and improved training, malposition of a central venous access device has been reduced but not eliminated.1 Confirming the position (or detecting malposition) of a central venous catheter may involve a conventional chest radiograph, transducing pressures or blood gas analysis on a sample from the catheter. These steps are usually used to determine arterial versus venous placement, but on occasions, the results do not confirm either.
This case highlights the utility of blood gas analysis as part of a structured approach. Using physiological first principles that the PO2 from the dialysis catheter is approaching that seen in the alveoli (PAO2=358 mm Hg based on alveolar gas equation and PaCO2=27 mm Hg), the tip must lie within or in contact with the pulmonary circulation.
Abnormal pulmonary venous drainage can be either total or partial and is the result of errors during embryological development. In the literature, the incidence of partial anomalous pulmonary venous connections (PAPVC) are reported to be between 0.4% and 0.7%.2 3 Although dependent on the shunt fraction, the presence of a PAPVC is usually asymptomatic and its diagnosis is usually incidental during other investigations.4
In the critical care setting, incidental diagnosis of a partial anomalous pulmonary venous connections during dialysis catheter insertion has been well described5–7 but the utility of blood gas analysis to provide early insight to the diagnosis less so.8 Furthermore, this case highlights the benefits of accessing interventional radiology to both clarify the exact position and relocation for patients with limited other access sites.
Learning points
Incidental diagnosis of a partial anomalous pulmonary venous connections should be considered when the dialysis catheter takes an unusual trajectory on chest X-ray.
Blood gas analysis is an important tool in the stepwise diagnosis of a malpositioned dialysis catheter.
Interventional radiology is a useful resource for confirming the exact position and relocation of catheters, especially in patients with limited access sites.
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank Dr Kendal Redmond.
Footnotes
Twitter @hvreynolds
Contributors Both authors contributed directly to the care of the patient and concept for the case report. HR contributed to the main write up and editing of the manuscript as well as obtaining images and consent from the next of kin. PSK contributed to editing the manuscript and supervision of the case report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.