Article Text

Statistics from Altmetric.com
Description
A 70-year-old man was referred to the pulmonary office for evaluation of a solitary lung nodule in September 2019. The patient was diagnosed with stage 1 adenocarcinoma of the rectum in November 2018 and underwent low anterior resection without any complications. No chemotherapy or radiation therapy was recommended. He underwent routine surveillance with combined tumour marker and radiological assessment every 3 months. A positron emission tomography (PET)-CT scan obtained in August 2019 revealed a PET-positive (standard uptake value (SUV) 3.2) right upper lobe (RUL) lung nodule, measuring 1.9×1.6 cm, abutting the mediastinal pleura (figure 1). The tumour marker, carcinoembryonic antigen level, was normal. The patient denied any fever, night sweats, weight loss, loss of appetite, cough, sputum production or haemoptysis. The patient was a never smoker. He denied any personal history of tuberculosis (TB) or exposure to patients with TB. His physical examination was unremarkable. Laboratory data was normal.

(A) Axial CT of the chest showing right upper lobe lung nodule (1.9×1.6 cm) abutting the mediastinal pleura (arrow). (B) The positron emission tomography CT scan revealed hypermetabolic activity in the nodule (arrow).
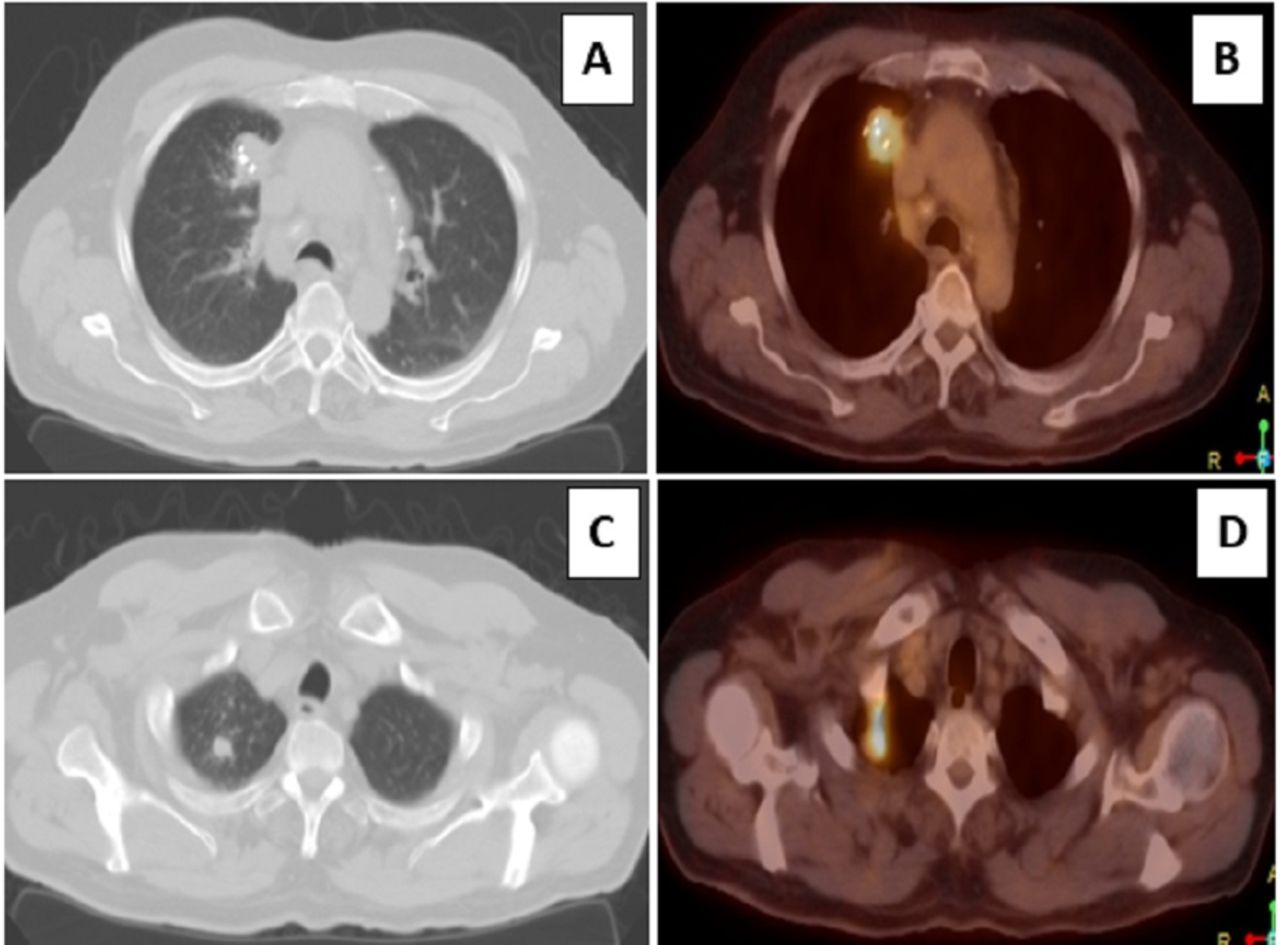
The patient underwent bronchoscopy with transbronchial lung biopsies, which were non-diagnostic. Surgical lung biopsy by video-assisted thoracoscopic surgery was performed in November 2019. Histopathological analysis of the lesion showed granulomatous inflammation with extensive areas of necrosis (figure 2). No malignancy was identified. The acid fast bacillus and Grocott-Gomori’s methenamine silver stains were negative for mycobacterial and fungal pathogens, respectively. There was no evidence of granulomatous or lymphocytic vasculitis. The patient was diagnosed with nodular sarcoidosis (NS). A repeat PET-CT in December 2019 demonstrated enlarging RUL lung mass (3.3×2.2 cm) with increasing SUV of 4.7 and a new nodule in the right apex with an SUV of 6.7 (figure 3).

Histopathological analysis of the surgical lung biopsy revealed loosely arranged sarcoid-like granuloma with extensive necrosis. No evidence of vasculitis was present.

Axial CT and corresponding PET-CT images of the right upper lobe nodules. The pre-existing nodule increased in size measuring 3.3×2.2 cm. Areas of calcification within the lesion was seen (A). The PET-CT showed higher SUV (4.7 from 3.2) (B). A new right apical nodule (C) with a SUV of 6.7. PET, positron emission tomography; SUV, standard uptake value.
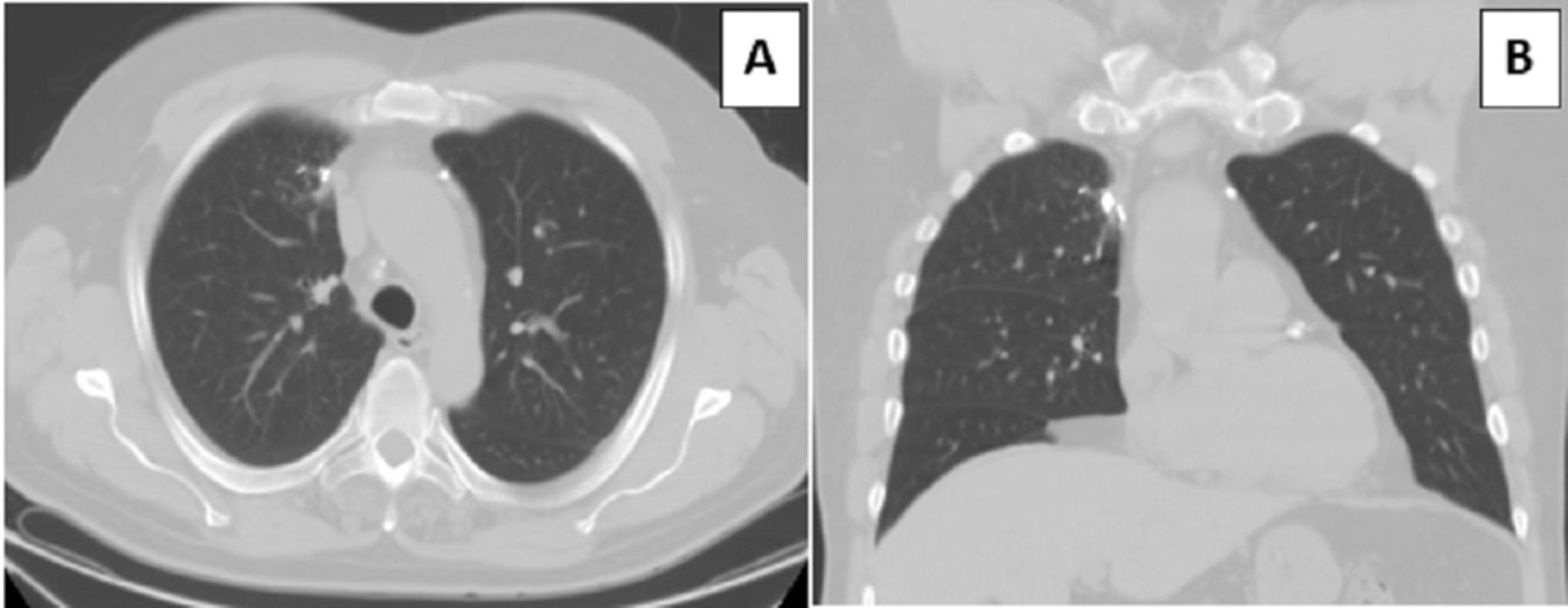
Although no malignancy was seen on the surgical lung biopsy specimen, given the enlargement of the existing lesion and development of a new lesion (both with PET positivity), the concern for metastatic disease existed. As NS is generally responsive to systemic corticosteroid therapy, a trial of prednisone was initiated. A CT scan obtained after a month of therapy with 20 mg of prednisone demonstrated complete resolution of both lesions (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CT chest, axial (A) and coronal (B) views showing complete resolution of both lung nodules. The calcification at the site of the first lung nodule was visible.
NS is an uncommon form of sarcoidosis. The prevalence of NS varies between 1.6% and 4% among all patients with sarcoidosis.1 In contrast to the typical sarcoid nodules, which measure 2–5 mm and are perilymphatic in distribution, nodules in NS are mass like, measuring 1–5 cm in diameter. The lesions are often confused with primary or metastatic pulmonary malignancy. Like classic sarcoidosis (CS), NS is more prevalent in women. However, the disease seems to have a predilection for Caucasians and is typically present before the age of 40 years.2
The presentation of NS is similar to CS. Patients may present with systemic and/or pulmonary symptoms. Many patients are asymptomatic and only brought to medical attention after incidental identification of lung nodule on chest imaging performed for another indication. Lungs are the most commonly affected organ. The exact incidence of extrapulmonary disease is unknown but likely similar to that of CS.3 4 Intrathoracic lymphadenopathy is seen in approximately 85% of patients.1 Due to the presence of activated T lymphocyte in granulomatous inflammation, the nodules in NS are metabolically active on PET scan.5 The PET positivity might further mislead the clinician towards a clinical diagnosis of malignancy.
The diagnosis of NS is made from biopsy and histopathological analysis of the affected organ. Unlike tightly packed monotonous sarcoid granuloma in CS, NS shows coalescing sarcoid like granuloma. The granulomas could be necrotising or non-necrotising. The extent of necrosis can vary from small punctated to large confluent areas. The incidence of necrosis in NS is about 14%.2 The presence of necrotising granuloma often raises the concern for fungal or mycobacterial disease, and exclusion of fungal and mycobacterial pathogens is crucial before making a confident diagnosis of NS.6
Another disease entity that may be challenging to differentiate from NS is necrotising sarcoid granulomatosis (NSG). Both entities may manifest with similar clinical and radiological findings. However, a diagnosis of NSG requires the presence of destructive granulomatous (rarely lymphocytic) vasculitis in addition to granulomatous inflammation and necrosis.7 8 It is crucial to emphasise that granulomatous vasculitis may also be present in NS, but it is not destructive.2 Vasculitic changes can be present in up to 14% of patients with NS.2
Like CS, spontaneous resolution can occur in both NS and NSG, a feature more common with NS than NSG. Both conditions are steroid-responsive. A complete response to steroids, in this case, reconfirmed the diagnosis of NS.8 NS should be considered in the differential diagnoses of PET positive lung mass, especially if a lobectomy is planned. Intraoperative frozen section analysis may prevent unnecessary removal of functioning lung parenchyma.
Learning points
Nodular sarcoidosis (NS) can present as a positron emission tomography positive pulmonary mass mimicking malignancy.
Histopathological analysis of NS typically demonstrates coalescing necrotising or non-necrotising sarcoid like granuloma without any significant granulomatous vasculitis. Some lesions might have extensive necrosis.
Mycobacterial and fungal diseases need to be ruled out before making a diagnosis of NS.
Frozen section analysis of solitary lung nodule/mass before lobectomy may prevent unnecessary removal of functioning lung parenchyma.
Ethics statements
Footnotes
Contributors SS, WHC, AB and BS were involved in the planning, collection of data, and preparation of the initial and final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer-reviewed.