Article Text

Statistics from Altmetric.com
Description
Cavitary optic disc anomalies can cause maculopathy. The most common of these associated with maculopathy is the optic disc pit. Very rarely, maculopathy can accompany optic disc coloboma. We report a case of combined cavitary disc anomalies (coloboma and disc pit) with maculopathy.
A 22-year-old young woman presented with decreased vision in the left eye (LE) for 6 months. The right eye (RE) had poor vision since childhood. Best corrected visual acuity was 2/60 in the RE and 6/24 in the LE. Fundus examination of the RE showed a retinochoroidal coloboma (RCC) involving the disc and macula (figure 1A) and the LE showed a cavitary defect involving inferior half of the disc with adjoining macular thickening and retinal pigment epithelium changes (figure 1B). Optical coherence tomography (OCT) scans through the left macula showed retinal schisis with foveal detachment (figure 1C).

(A) Fundus photograph of the right eye showing a coloboma involving the disc and inferior retinochoroidal layer. (B) Left eye shows a cavitaryanamoly of the inferior half of the optic disc with adjoining retinal pigment epithelium changes and macular thickening. (C) Optical coherence tomography scan through the left macula showing retinal schisis in outer layers and subretinal fluid.
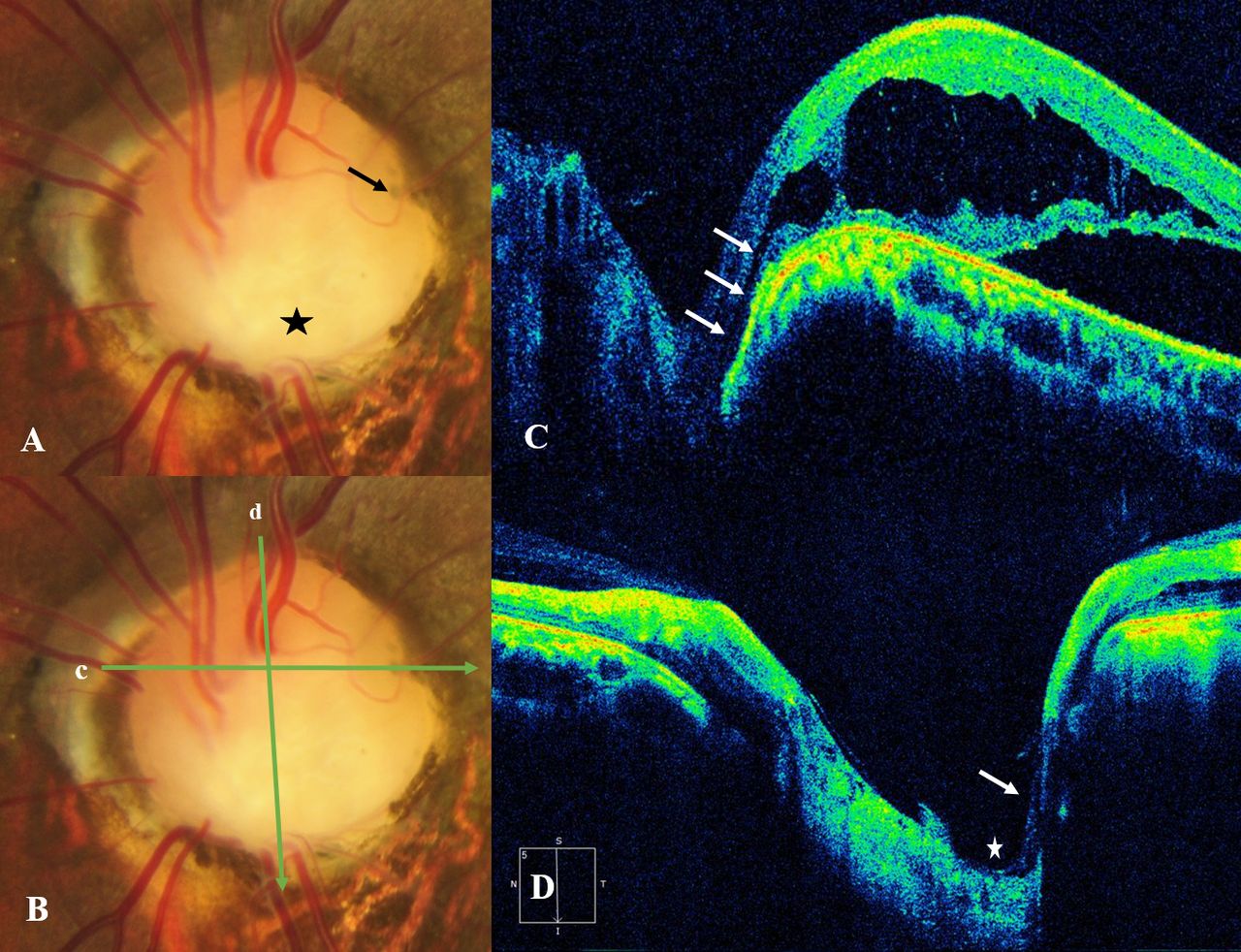
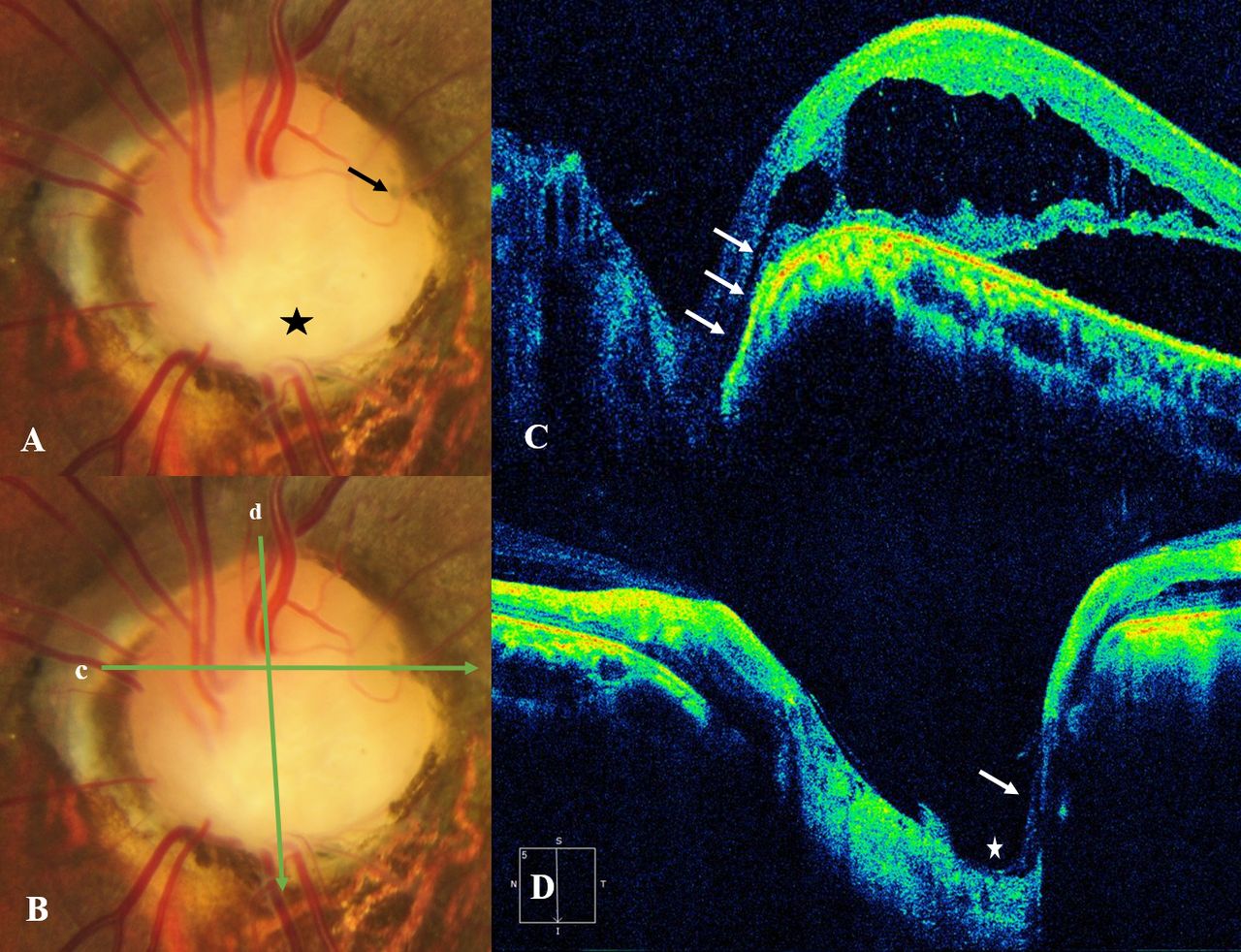
Closer observation of the left optic disc revealed a circular greyish focal dip on the temporal margin suggestive of a pit (figure 2A, arrow). OCT scans through the optic disc in this region showed a narrow slit-like tract extending from the schitic retina to the depths of the lamina cribrosa (figure 2B,C, arrows). Vertical line scan through the larger cavitary defect of the left optic disc showed a widened scleral canal, posteriorly displaced lamina cribrosa with dysplastic retina lining the wall (figure 2D, arrow) consistent with a colobomatous defect. Hence, a diagnosis of LE optic disc pit maculopathy with disc coloboma was made.
{kind=link}
{kind=link}
(A) Colour photograph of the left optic disc showing a sharply delineated, colobomatous excavation of the inferior half of the disc (asterisk) and a pit which is seen as a greyish focal depression on the temporal edge of disc (arrow). (B) The positions of the horizontal and vertical line scans corresponding to (C) and (D) are shown. (C) Horizontal line scan through the pit showing a narrow tract (arrows) extending deep into the lamina cribrosa. (D) Vertical scan though the disc showing an excavation in the inferior portion of the disc (asterisk) with herniation of the dysplastic retina (lacy appearance) (arrow).
Optic disc pits are congenital cavitary anomalies of the disc which can present in isolation or in combination with an RCC.1 2 The coexistence of a disc coloboma with a pit is a rare entity. Maculopathy in such cases may develop either from disc pit or rarely from the coloboma.2 3 In a study on cavitary disc anomalies using swept source OCT, the author observed that the anatomical and physiological barrier between the subarachnoid space and the vitreous cavity is compromised by the presence of pits and colobomatous defects in the disc. In the present case, the presence of both these defects in close proximity could have increased the risk of developing maculopathy.
Optic disc colobomas need to be differentiated from acquired causes like glaucomatous cupping. A characteristic bowl-shaped white glistening defect with well-delineated edges in an abnormally large disc should raise suspicion of a disc coloboma. Dysplastic retina herniates into the excavation and takes on a lacy appearance on OCT.1 The macular thickening in cavitary disc anomalies presents with retinal schitic changes which may misdiagnosed as macular oedema of retinal vascular origin. Careful evaluation of the disc for pit lesions and demonstration of anatomical defects using OCT helps in arriving at the correct diagnosis. Vitrectomy with or without tamponade and laser have been shown to be successful in resolving maculopathy changes secondary to optic disc pits.4–6
This case emphasises the need for a meticulous imaging of the optic nerve head in cases with cavitary disc anomalies and maculopathy to arrive at the correct diagnosis and plan appropriate management.
Learning points
Cavitary disc anomalies can present with varied combinations including coloboma and pit.
Meticulous imaging of the disc and macula is needed to demonstrate morphological changes and hence correct diagnosis.
The management of such cases changes as many of the conditions are treatable.
Ethics statements
Patient consent for publication
Footnotes
Contributors RH evaluated the case. NCK prepared the manuscript and relevant literature search. PG reviewed the draft and finalized it.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.