Article Text

Statistics from Altmetric.com
Description
Left ventricular (LV) pseudoaneurysm is a rare but potentially fatal complication of myocardial infarction (MI) which needs to be differentiated from true LV aneurysm.1 Most of the LV pseudoaneurysms post MI are located at the inferior and posterolateral wall (82% of all post MI pseudoaneurysms).1 2 We hereby present an anterolateral LV pseudoaneurysm post MI, which makes it even a rarer entity.
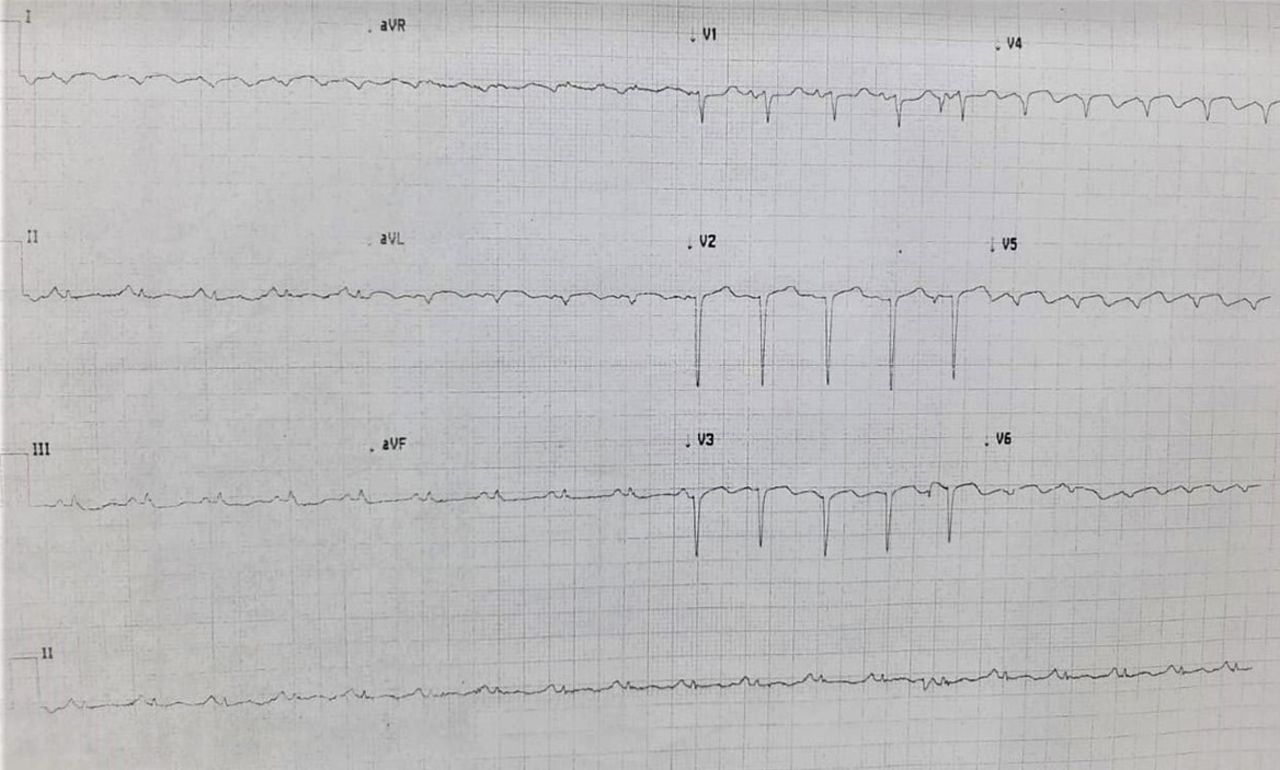
A 78-year-old frail woman, a known case of diabetes mellitus type 2 and hypertension, presented to the emergency department with worsening dyspnoea of 2 weeks’ duration. She had a history of chest discomfort 1 week prior to the onset of dyspnoea, which resolved with some medication prescribed by the local doctor. On presentation, she was orthopneic with saturation of 82% at room air and had mean arterial pressure of 76 mm Hg. She had a gallop rhythm with bilateral widespread crepitations in the chest. N-terminal pro-B-type natriuretic peptide, troponin T and creatine kinase MB were 6980 pg/mL (normal <300 pg/mL), 0.56 ng/mL (normal <0.4 ng/mL) and 42 IU/L (normal 5–25 IU/L), respectively. Reverse transcription PCR for COVID-19 was negative. Transthoracic 2D echocardiography revealed an ejection fraction of 20% with a large anterolateral pseudoaneurysm which was confirmed on 3D echocardiography (figure 1A–D). Her electrocardiogram revealed QS in V1–V6, I and aVL (figure 2). She was managed with antiplatelets, anticoagulation, non-invasive ventilation and diuretics. After haemodynamic stabilisation, she was taken up for coronary angiography and ventriculography. Coronary angiography revealed diffuse disease of the left anterior descending artery. Anterolateral pseudoaneurysm was confirmed on left ventriculography (video 1) and cardiac MRI (video 2). The patient was offered surgery; however, the relatives and the patient wanted medical management only. At 3 months’ follow-up, the patient is alive and can do activities of daily living with minimal dyspnoea.

Transthoracic echocardiography (TTE) 2D, parasternal long axis (PLAX) and apical four-chamber (A4C) views showing pseudoaneurysm (A,B). TTE 3D, PLAX and A4C views showing pseudoaneurysm (C,D). Coronary angiography showing diffusely diseased left anterior descending artery (E).

{kind=link}
{kind=link}
Twelve-lead Electrocardiogram.
LV pseudoaneurysm, post MI, has a reported incidence of less than 2%, with inferior and posterolateral wall being the most common locations (82% of all MI), which makes LV anterolateral pseudoaneurysm extremely rare.1 2 It may also occur after cardiac surgery, endovascular interventions and trauma.2 The most common presentation is dyspnoea (15%) followed by chest pain (13%), arrhythmias/syncope (10%) and systemic embolism (6%).1 2 While 10% of the cases may be discovered incidentally, it can also present with cardiac tamponade and sudden cardiac arrest.2 Unlike the true aneurysm, it carries a very high risk of rupture (30%–45%).3 4 In majority of the cases, transthoracic echocardiography is sufficient for diagnosis. Besides the typical location, neck diameter ratio of ≤0.7 favours pseudoaneurysm on imaging.3 4 Since our patient had anterolateral pseudoaneurysm which is very rare, we did contrast ventriculography and cardiac MRI to confirm the diagnosis and plan a possible surgical approach.3–5 Most symptomatic pseudoaneurysms require urgent invasive management; the mortality reaches 50% on medical therapy, which is halved with surgical intervention.3 4 In patients with high surgical risk, percutaneous closure of LV pseudoaneurysms can be tried, provided it is anatomically feasible.6
Our patient had a post MI LV anterolateral pseudoaneurysm which is rare and had a relatively less aggressive course, though long-term follow-up is awaited. In atypical cases, multimodality imaging may be required to confirm the diagnosis.
Learning points
Left ventricular pseudoaneurysm is a rare, but potentially fatal complication of myocardial infarction, which requires differentiation from true aneurysm.
Multimodality imaging may sometimes be required to differentiate the pseudoaneurysm from true aneurysm and to plan the surgical management.
Ethics statements
Footnotes
Twitter @AnilKumaroo7
Contributors NK: Data collection, literature review and writing the original draft. PP: Planning, conceptualisation, supervision, final review and editing. AKC: Data collection, literature review and writing the original draft. YPS: Planning, conceptualisation, supervision, final review and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer-reviewed.