Article Text

Abstract
We report a case of a ventricular septal rupture (VSR) which occurred during coronary artery bypass grafting (CABG) operation. The procedure took place 5 days after ST-elevation myocardial infarction of the inferior wall. The VSR repair was not performed at the time of the CABG operation. The intention was to wait until scar formation occurs to facilitate the repair. The patient was supported with venoarterial extracorporeal membranous oxygenation (VA-ECMO) and additional intra-aortic balloon pump (IABP) on intensive care unit. Ten days after CABG the patient underwent a successful VSR repair and 5 days later was weaned from VA-ECMO. He was discharged from hospital 6 weeks after the initial CABG. This case report underlines the importance of VA-ECMO and a multidisciplinary approach with frequent examination of haemodynamic state in the treatment of patients with mechanical complications of myocardial infarction who are not suitable for immediate repair.
- heart failure
- ischaemic heart disease
- cardiothoracic surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Ventricular septal rupture (VSR) is nowadays a rare complication after ST-elevation myocardial infarction (STEMI). To our knowledge, this is the first case report which describes a VSR which occurred during coronary artery bypass grafting (CABG).
Case presentation
Introduction
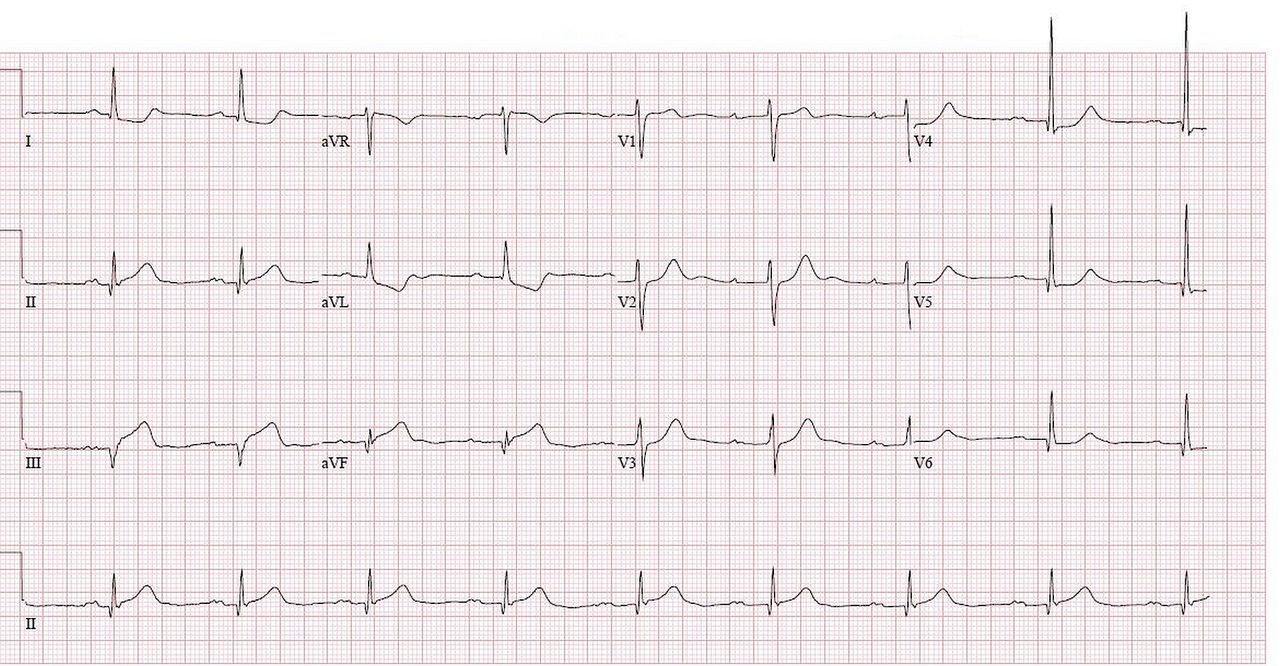
A 62-year-old man presented to our hospital with STEMI of the inferior wall (ST elevations in II, III and aVF) (figure 1). Cardiac enzymes were significantly elevated (Creatine kinase-MB (CK-MB) of 214 μg/L, normal range: 0–7 μg/L). Coronary angiography (CAG) revealed an occlusion of the right coronary artery and a significant distal left main stem stenosis. A spontaneous resolution of ST elevation was observed during the CAG procedure.
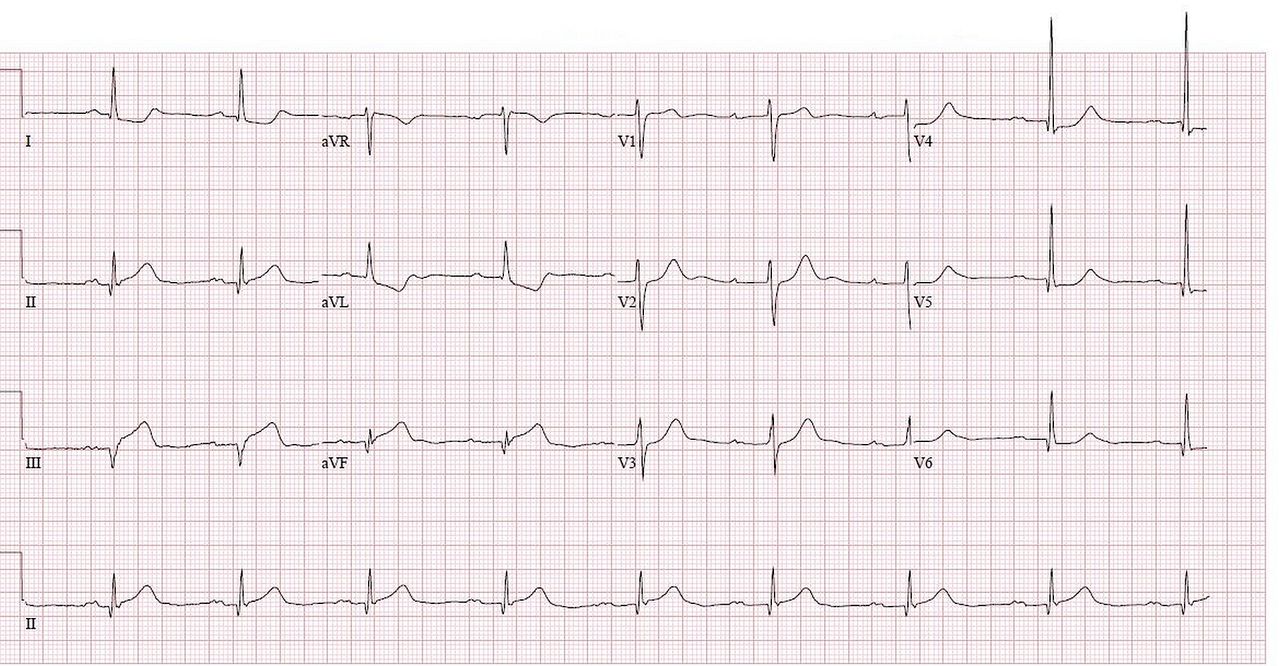
ECG at the moment of presentation at het hospital. ST elevation in II, III and aVF with reciproke depression in aVL, leading to the diagnosis of inferior ST-elevation myocardial infarction.
The patient did not have any symptoms of acute heart failure. Cardiac ultrasound showed moderate left ventricular dysfunction with akinesia of the inferior wall. The patient was discussed in the heart team and accepted for urgent CABG.
Treatment
Coronary artery bypass grafting
Five days after STEMI the patient underwent on-pump CABG. Transoesophageal echocardiography (TEE) after induction of anaesthesia showed no left-to-right shunt. The left internal mammary artery (LIMA) was anastomosed with the first diagonal and the left anterior descending artery. The obtuse marginal branch and posterior descending artery were grafted with the left radial artery, which was proximally anastomosed to the LIMA in a Y-graft fashion. After removing the aortic cross-clamp severe distension and dysfunction of the right ventricle (RV) were observed. TEE revealed a VSR with left–right shunt through the ventricular septum (figure 2). We concluded that direct closure of the VSR in this situation with friable tissue in the recently infarcted myocardium and diffusely infiltrated hematoma on the inferior wall carried a very high risk of repair failure. It was decided to postpone the repair of the VSR and support the patient with venoarterial extracorporeal membranous oxygenation (VA-ECMO) (via the left femoral vein and artery) until the scar forms in the infarcted area. The patient was then transferred to the intensive care unit (ICU). The plan was to reoperate the patient after around 10 days, expecting better demarcation of the infarcted septum.
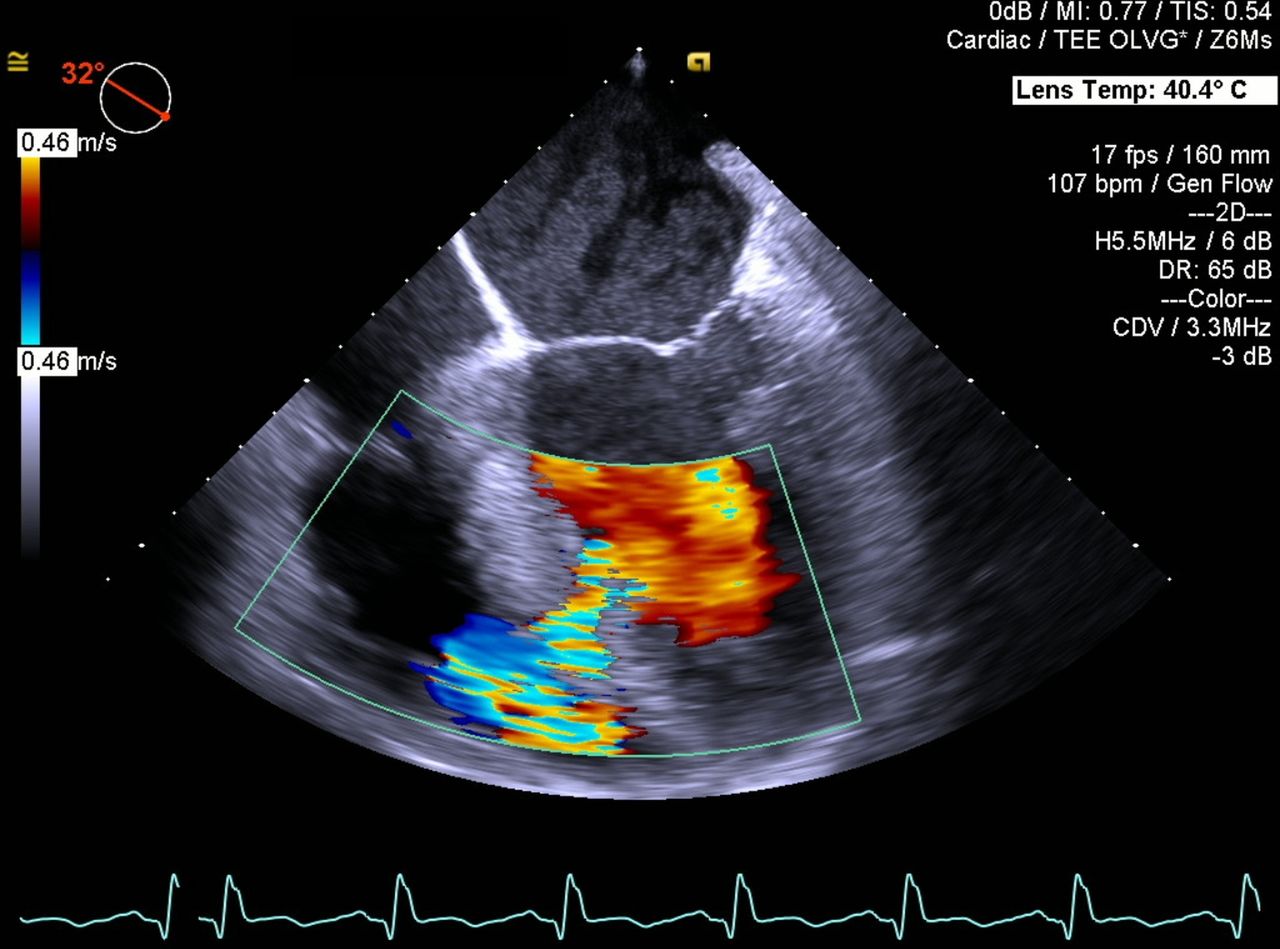
Transoesophageal echocardiography showing ventricular septal rupture with Doppler flow from left to right ventricle.
ICU stay
The patient was admitted to the ICU with VA-ECMO (4.7 L/min blood flow, 3.5 L/min gas flow), enoximone, amiodarone and low-dose norepinephrine intravenous continuously (for all dosages and parameters see figure 3). The patient was haemodynamically stable. There were no problems with oxygenation and ventilation on respiratory support by mechanical ventilation via an oral endotracheal tube.

Timeline and table with oxygenator, venoarterial extracorporeal membranous oxygenation (VA-ECMO) and intra-aortic balloon pump (IABP) settings and doses of inotropics. ICD, implantable cardioverter defibrillator; PEEP, Positive end-expiratory pressure; STEMI, ST-elevation myocardial infarction; VSR, ventricular septal rupture.
The next morning TEE was performed as part of daily routine in ECMO patients in ICU and because of loss of pulsatility in the arterial pressure curve. The TEE revealed that the aortic valve (AV) was constantly in the closed position.
The blood flow on VA-ECMO was reduced to 3.7 L/min, AV opened and pulsatility returned. A couple hours later AV was not opening again. Blood flow was further reduced to 2 L/min. However, in the meantime the renal function began to deteriorate due to low cardiac output. It was decided to insert an intra-aortic balloon pump (IABP) via the right femoral artery. The IABP supported every heartbeat (1:1 mode). After insertion of the TEE probe opening of the AV in systole and normal flow in the aortic root was observed. In the meantime the VA-ECMO flow was increased from 2 L/min up to 3 L/min. This, in turn, resulted in less opening of the AV and less flow in the aortic root on TEE. A good equilibrium was found at an ECMO flow of 2.4 L/min.
TEE revealed dilated RV with poor function. Iloprost, a prostacyclin analogue which leads to selective vasodilatation of pulmonary circulation, was started to reduce the right ventricular afterload. Enoximone was continued to support RV contractility and decrease the afterload of both ventricles. Low-dose norepinephrine was restarted to maintain adequate mean arterial pressure. These doses of vasopressin and inotropes together with IABP 1:1 made it possible to increase VA-ECMO flow till 2.8–3.0 L/min to maintain adequate systemic circulation.
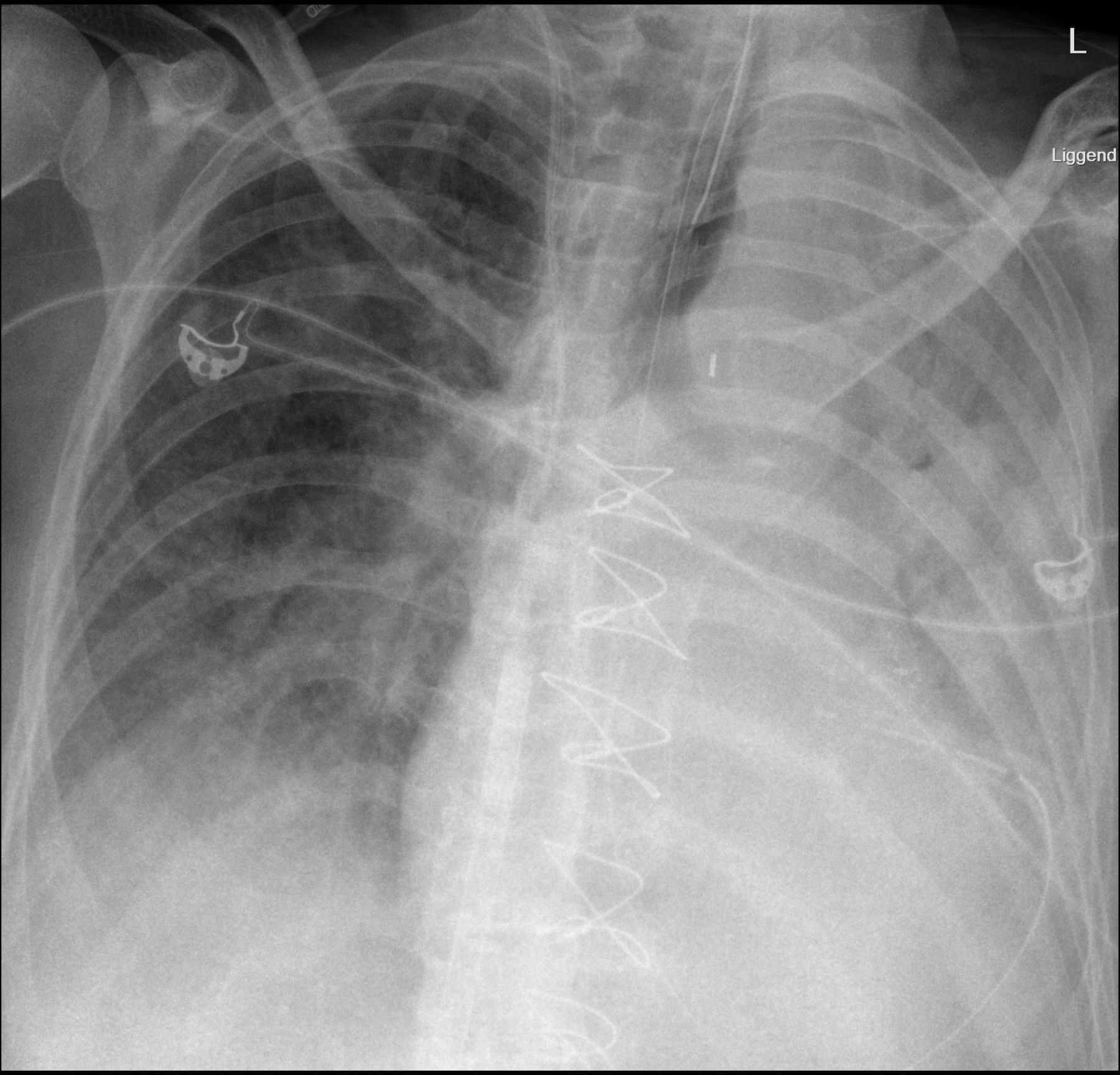
In the meantime, the patient developed pulmonary problems due to intra-bronchial blood clots, which caused complete atelectasis of the left lung (figure 4). Bronchoscopy was performed several times with removal of clots. To ensure sufficient oxygenation FiO2 of 85% and positive end-expiratory pressure (PEEP) of 7 cm H2O was needed, the patient was proned at night to reduce perfusion/ventilation mismatch. High PEEP levels were not used to avoid increase of RV afterload.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Atelectasis of the whole left lung.
Ventricle septum repair
Ten days after the initial CABG, the patient underwent surgical correction of the VSR. The operation was performed via resternotomy and standard extracorporeal circulation with bicaval vein cannulation and total bypass. The heart was arrested using cold blood cardioplegia and the posterior left ventriculotomy was performed parallel to the posterior descending coronary artery. Inspection showed VSR with distinct demarcation of infarcted tissue. A bovine pericardial patch was used to cover the ventricular septal defect (David exclusion technique). Due to demarcation, it was possible to place the stitches of the pericardial patch in solid, viable tissue. The ventriculotomy was then closed with two additional bovine pericardial patches (sandwich technique) with Teflon felt strips. The patient was weaned from the cardiopulmonary bypass and support with a new ECMO system was continued. The postoperative TEE showed no residual left–right shunt.
Outcome and follow-up
ICU stay after VSR repair
The patient was readmitted to the ICU after operation with VA-ECMO with a blood flow of 3.6 L/min and IABP support (1:1). Postoperative TTE showed severe dysfunction of the left ventricle (LV). Oxygenation was poor at that time, increasing PEEP led to desaturation due to increase of perfusion–ventilation mismatch. Hypoxemia was caused by a combination of atelectasis and pleural effusion next to increased RV afterload. The patient was proned again for two nights with good result. Every day, cardiac function was evaluated by TTE and treatment policies were discussed and determined in a multidisciplinary team consisting of an intensivist, cardiologist and cardiothoracic surgeon. Five days after VSR repair the patient was weaned from VA-ECMO. IABP was left in situ to support the poor LV. Two days after removal of VA-ECMO, the patient was haemodynamically stable enough to remove the IABP. TTE showed poor left ventricular function (ejection fraction of 20%) and a moderate right ventricular function. Ten days after the reoperation patient was extubated. The patient was suffering from ICU acquired weakness and required intensive rehabilitation programme. Twenty-three days after the reoperation he was transferred to the regular cardiac surgery ward. For secondary prophylaxis of ventricular tachycardia/fibrillation a 1-lead ICD was placed. The patient was transferred to a rehabilitation centre after 19 days on the cardiothoracic ward, where he spent additional 2 months before being discharged home. The patient is currently doing well at home.
Discussion
A VSR after acute myocardial infarction (AMI) is nowadays a relative rare complication after AMI due to the advent of emergent reperfusion strategies. VSR has an incidence between 0.17% and 0.31% of patients presenting with AMI.1
We present a rare case of intraoperative VSR. The most likely cause of the intraoperative rupture was a combination of the weakening of the myocardium caused by the infarction and an unavoidable manipulation that occur during an open heart surgery.
Surgery is the recommended treatment for ventricle septal rupture. In the early phase infarcted myocardium is fragile. Collagen is microscopically detectable in infarct tissue usually 7 days after the infarction and fibrous tissue replace necrotic myocytes completely around day 28.2 Delayed surgery is associated with lower mortality, possibly due to improved stability of the cardiac tissue.1 Delayed surgery should be performed in patients well responding to aggressive heart failure therapy.3 When medical therapy fails, mechanical support (IABP or VA-EMCO) can be used as bridge to delayed surgery. Liebelt et al describe a retrospective cohort of 14 patients after VSR. Usage of both IABP and ECMO was more common for a longer duration in the survival group (four patients).4 Significant prospective or retrospective studies evaluating ECMO in the treatment of VSR are not available. The efficacy of ECMO is suggested in several case reports.5–8 This case report demonstrates the successful use of ECMO and IABP in the treatment of VSR after CABG.
Patient’s perspective
It is extraordinary that I survived the ventricle septal rupture, surgical repair, period on the venoarterial extracorporeal membranous oxygenation and postoperative stay on the intensive care unit. Mentally my family and I are still processing this period. Currently I am at home and I am still making progress with my rehabilitation. I am doing exercise on my hometrainer on a daily base.
Learning points
We discern three major learning points in this complex postoperative course of our patient.
The debatable optimal timing of ventricular septal rupture repair: We were afraid of the risk of an unsuccessful repair of the VSR due to frail tissue immediate after rupture. On the other hand, the ‘watchful waiting’ period with VA-ECMO in situ can lead to other complications including infection, thromboembolic events, bleeding and irreversible right ventricle failure due to volume overload by persisting VSR. In our case, the delayed surgery 10 days after VSR seemed to be optimal timing for reoperation. No major complications occurred during the ‘watchful waiting’ time. Intraoperatively, there was a visible demarcation of infarct tissue observed, which served as a firm edge for the stitches of bovine pericardial patch.
The treatment of this kind of complex haemodynamic shock with a VSR and peripheral VA-ECMO: Frequent evaluation of cardiac function was essential in the treatment of a patient with VSR and left–right shunt. ECMO flow needs to be adjusted frequently based on the echocardiographic findings. When adaptation of ECMO flow is not enough to optimise the haemodynamic status of the patient, the implementation of possible additional assist devices should be considered. In our patient, the IABP was inserted to decrease the left ventricular afterload. This, in turn, facilitated the blood flow from the LV to the aorta and decreased the left–right transseptal shunt. Thanks to IABP, the ECMO flow could be kept at a level that provided the patient with optimal peripheral perfusion.
The optimal ventilation strategy during haemodynamic shock with left-to-right shunt: Achieving optimal oxygenation can be cumbersome because increasing PEEP result in elevation of RV afterload. One of the possibilities to improve perfusion/ventilation mismatch in the setting of relatively low PEEP could be ventilation in prone position.
This case report shows the importance of a multidisciplinary approach with frequent examination of haemodynamic state to successfully treat a patient with VSR after myocardial infarction who is supported with VA-ECMO.
Ethics statements
Patient consent for publication
Footnotes
Contributors CLK wrote the surgical sections together with TPP and WS. Postoperative sections were written by CLK, AB and TPP. All authors wrote the Discussion and drafted, reviewed and were in agreement on the final product of the manuscript and its contents.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.