Article Text

Statistics from Altmetric.com
Description
A 64-year-old hypertensive man presented with angina on walking around 500 meters for the last 9 months. On examination, his blood pressure was 130/70 mm Hg and the rest of the general physical and cardiac examination was unremarkable. His 12-lead electrocardiogram was within normal limits and the transthoracic echocardiogram revealed a structurally normal heart with a left ventricular ejection fraction of 60%. A treadmill test (TMT) was positive for inducible ischaemia at moderate workload and a subsequent angiogram performed revealed normal left coronary circulation and proximal right coronary artery (RCA) chronic total occlusion (figure 1A).
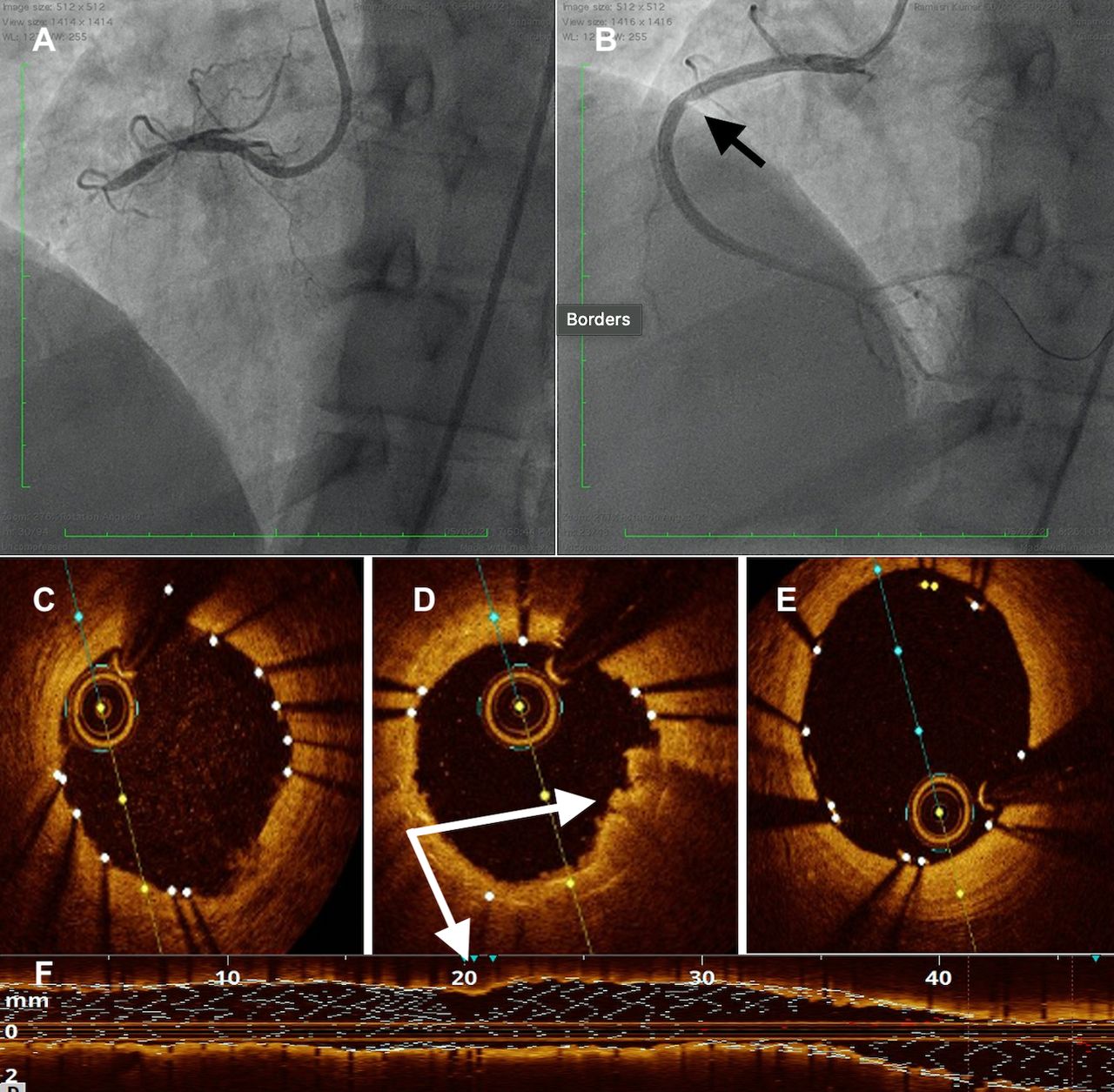
(A) Coronary angiogram in LAO cranial projection showing chronic total occlusion of right coronary artery. (B) Following deployment of two overlapping drug-eluting stents, intraluminal haziness is obvious at the overlap site (black arrow). The distal (C) and the proximal (E) portions of the stent are well apposed on optical coherence tomography (OCT) images. The OCT image (D) corresponding to the haziness on the angiogram shows evidence of thrombus and plaque protrusion. Underlying stent struts are obscured (F) due to the overlying thrombus (white arrows). LAO, left anterior oblique
He remained symptomatic with angina despite optimal medical therapy for 3 months, and subsequently taken up for percutaneous coronary intervention (PCI). He was loaded with clopidogrel 300 mg 10 hours before the procedure. After successful wire passage and pre dilatation, two long overlapping drug-eluting stents (3×32 and 3.5×38 mm; Promus Premier, Boston Scientific, Natick, Massachusetts, USA) were placed from distal to proximal RCA. After postdilatation at 18 atm pressure with a 3.5×12 non-compliant balloon, a subsequent angiogram revealed intraluminal haziness at the stent overlap site (figure 1B; video 1) with Thrombolysis in myocardial infarction 3 flow distally. He remained haemodynamically stable in sinus rhythm without any arrhythmias. Differential diagnoses included stent fracture, thrombus or dissection.
Optical coherence tomography (OCT) (DragonFly Optis imaging catheter, St. Jude Medical, MA, USA) has previously been shown to guide the physician in decision making and have a positive impact during PCI.1 OCT was performed in the index case and revealed (figure 1C–F) a thrombus and plaque protrusion at the site and a signal drop-off was seen such that the underlying stent struts could not be visualised (figures 1D and 2A; video 2. There was no evidence of dissection. Since a thrombus can obscure the underlying stent due to attenuation,2 3 the possibility of underlying stent fracture could not be ruled out. To rule out stent fracture with certainty, StentBoost (Phillips Healthcare, Best, Netherlands) was performed which revealed adequate stent expansion and no evidence of stent fracture (figure 2B). StentBoost has previously shown a good correlation with intravascular ultrasound to evaluate stent expansion and identify and stent strut fracture or under expansion.4–6 Subsequently, he received tirofiban infusion at 0.15 mcg/kg/min for 8 hours. He had an uneventful perioperative and postoperative period and remained free of any ischaemic or bleeding events. There was no increase in cardiac biomarkers from the baseline. He was discharged 2 days later. Currently, the patient is asymptomatic at 6 months of follow-up. A recent TMT was negative at a high workload. This case highlights the synergistic effects of OCT and StentBoost in the evaluation of poststenting complications. It brings precision in the field of coronary intervention and guides management strategy.

{kind=link}
{kind=link}
Three-dimensional optical coherence tomography image showing a signal drop off at the site of haziness and raising the possibility of underlying strut fracture (A). However, StentBoost images acquired after balloon placement, show smooth outlining of the stents with adequate overlap and without any evidence of stent fracture (black arrow) (B).
Patient’s perspective
Nine months ago, I felt a little worried when the doctors told me that they were concerned about some blood clot at the time of my stenting, and I had to stay in hospital for an extra couple of days. Thanks to their efforts, I am healthy now and able to perform all my work without any symptoms.
Learning points
Revascularisation is indicated for chronic total occlusion if symptomatic despite optimal medical therapy.
Thrombus can attenuate the underlying stent struts and make its assessment difficult during intravascular imaging with optical coherence tomography.
StentBoost offers a suitable alternative for rapid identification of any stent-related pathology including stent expansion and stent fracture.
Acknowledgments
Mr Ramneek Atrii for providing the optical coherence tomography images.
Footnotes
Contributors AB contributed to conceptualisation, methodology, investigation, supervision, original draft preparation, reviewing and editing. PP and KM contributed to original draft preparation, reviewing and editing. YPS contributed to supervision, reviewing and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.