Article Text

Statistics from Altmetric.com
Description
A 65-year-old man experienced sudden onset of abdominal pain while working on his farm without significant trauma. He heard a ‘pop’ sound, followed by abdominal pain, lightheadedness and diaphoresis. He has a history of polycythemia vera (PV) and chronic severe splenomegaly, treated with roxulitinib. He was diagnosed with acquired von Willebrand syndrome 6 years earlier after prolonged bleeding from a tooth extraction.
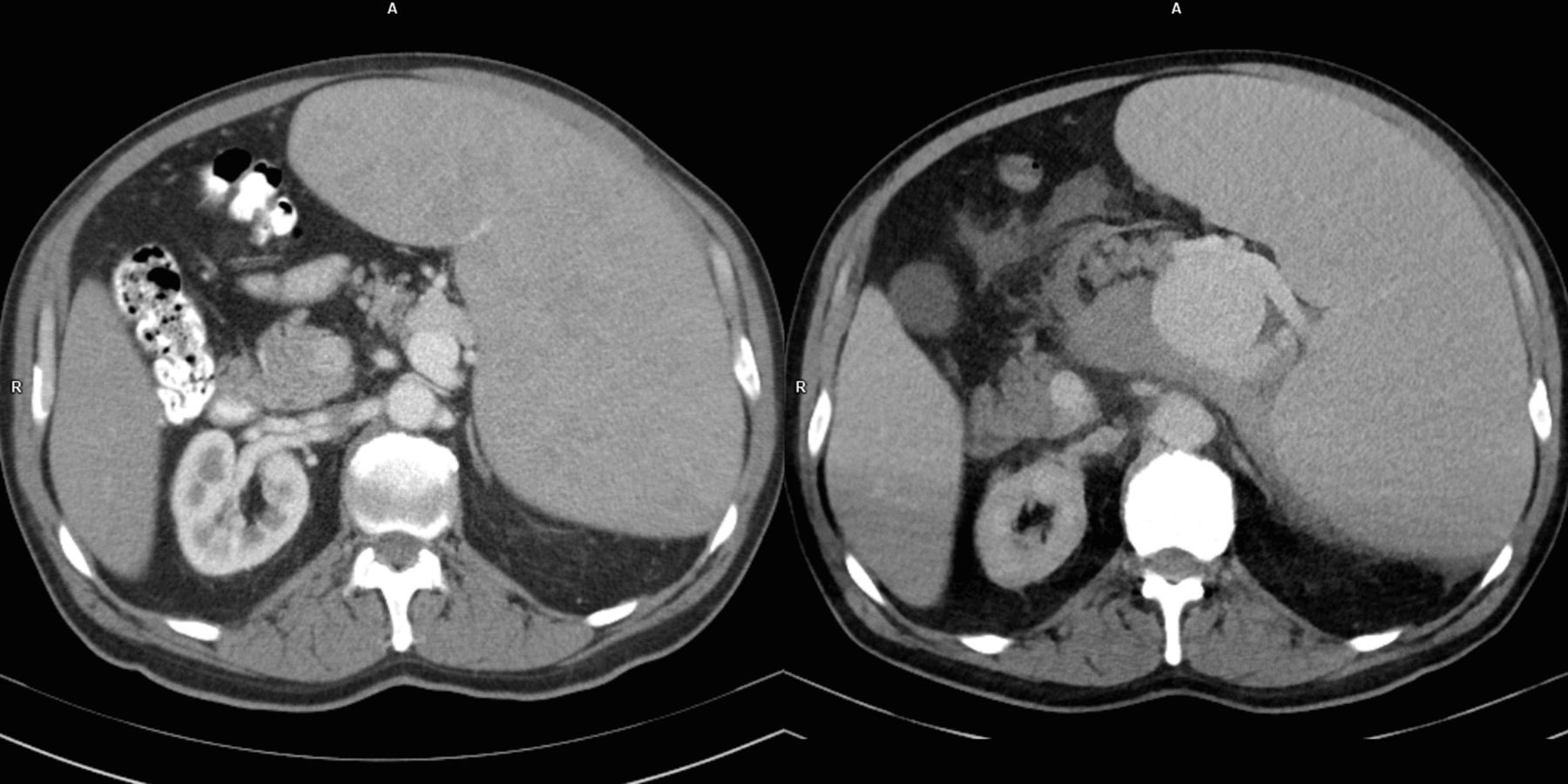
On presentation to the local hospital, the patient’s symptoms had nearly resolved. He underwent an abdominal CT scan demonstrating a 4.8 cm splenic artery aneurysm, increased from 1.8 cm on prior CT 6 years earlier (see figure 1), now with surrounding hemorrhage in the mesentery and lesser peritoneal sac compatible with early rupture (see video 1). Hemoglobin was downtrending to 73 g/L on immediate transfer to tertiary medical center.

{kind=link}
Comparison of prior abdominal CT 6 years earlier (left) and current abdominal CT (right) demonstrates marked interval enlargement of splenic artery aneurysm with appearance of surrounding hemorrhage. Severe splenomegaly is noted on both examinations.
The patient received blood transfusions and von Willebrand concentrate shortly after evaluation. He underwent emergent splenic artery angiogram with coil embolization in the operating room. At the conclusion of this procedure, increased abdominal distention and hypotension were noted. Exploratory laparotomy demonstrated massive hemoperitoneum, and open splenectomy was performed. After a complicated postoperative course, the patient recovered and was discharged home several weeks later.
Splenic artery aneurysms (SAA) are the most common visceral artery aneurysms, with causes including pregnancy/multiparity, hypertension, portal hypertension, connective tissue disease, fibromuscular dysplasia and atherosclerosis.1–3 While the vast majority of SAA are asymptomatic, the rupture rate is 2%, with mortality as high as 36%.1 Sudden onset of left upper quadrant pain and hemodynamic instability is a prototypical presentation of rupture. As was a concern in this patient, the ‘double-rupture’ phenomenon has been described, where patients transiently stabilize (due to tamponade of hemorrhage in the lesser peritoneal sac), followed by subsequent circulatory collapse (when hemorrhage extends to the peritoneal cavity).2 Conventional treatment options include surgical excision or ligation, while transcatheter embolization has gained favour.1–3 Endovascular therapy should be considered for asymptomatic aneurysms of 2 cm or larger.
PV is a myeloproliferative neoplasm associated with increased red blood cell mass and splenomegaly. Primary goals of management are to limit the risk of arterial and venous thrombosis using antiplatelet therapy, phlebotomy, interferon therapy or Jak1-2 inhibitors.4 Less common hemorrhagic complications have also been described in PV,5 related to underlying thrombotic events, antiplatelet medications or acquired von Willebrand syndrome. Although less frequent than with other lymphoproliferative and myeloproliferative neoplasms, acquired von Willebrand syndrome has been described in 12% of patients with PV, associated with higher platlet counts.6 This may predispose to mucosal and cutaneous bleeding, prolonged bleeding after surgical/dental procedures and occasionally major bleeding events.
There is no established association between PV and development of SAA. However portal hypertension is associated with increased risk of SAA (estimated 7%–20% prevalence of SAA in cirrhosis3), and up to 13% of patients with PV may have associated portal hypertension.7 Pathogenesis of SAA in portal hypertension may relate to increased splenic blood flow volume,8 and similar flow-related phenomena may have been present in this patient related to his severe splenomegaly.
Patient’s perspective
I was inside a grain bin lifting an auger, and all of the sudden I got dizzy and started sweating. I knew right away something wasn't right. After an hour or two, I felt better, but we still decided to go get checked out. My wife thought I was having a heart attack.
Learning points
Although the vast majority of splenic artery aneurysms are asymptomatic, rupture carries a high mortality rate, and preventive treatment of aneurysms >2 cm is paramount.
Acquired von Willebrand syndrome is associated with risk of hemorrhagic complications in polycythemia vera and is seen in patients with higher platelet counts.
Splenic artery rupture may present with a double-rupture phenomenon, where patients transiently stabilize before worsening hemodynamic status due to increased intraperitoneal haemorrhage.
Ethics statements
Footnotes
Contributors All authors were involved in conception of the case. NLL wrote the initial draft of the manuscript and assisted in revising and final approval of the manuscript. FAV and MJK assisted in drafting, revising and final approval of the manuscript. MJK prepared images and obtained informed consent from the patient.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.