Article Text

Statistics from Altmetric.com
Description
A 78-year-old man presented with moderate lens opacity and end-stage dry age-related macular degeneration (AMD) with visual acuity of logMAR 0.7 and 1.6 for right and left eyes, respectively. He was tested with an external telescope simulator device, showing an improvement of 20 letters and 2 letters for right and left eyes, respectively. He consented for right cataract extraction and insertion of an Implantable Miniature Telescope (IMT, by Dr. Isaac Lipshitz, VisionCare Ophthalmic Technologies, California, USA). The surgery was conducted under regional anaesthesia. Routine small-incision phacoemulsification was followed by IMT implantation into the capsular bag via a 12 mm corneal limbal incision, peripheral iridectomy formation and corneal closure with interrupted 10/0 nylon sutures (figure 1A).
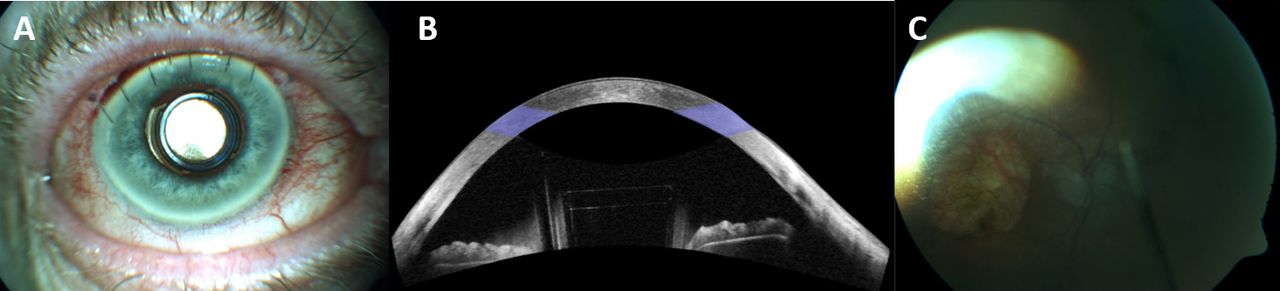
(A) Anterior segment photograph (FF450plus, Carl Zeiss MediTec, Dublin, California, USA) showing IMT device in the capsular bag and superior corneal sutures. (B) Anterior segment OCT (Cirrus 5000, Carl Zeiss MediTec) showing position of the IMT optic placed in the pupil margin with adequate lens-endothelial clearance. (C) Colour fundus photograph (FF450plus, Carl Zeiss MediTec) through the IMT demonstrating visualisation of the optic nerve head and macula. IMT, implantable miniature telescope; OCT, optical coherence tomography.
Best-corrected visual acuity (BCVA) in the IMT-implanted eye was measured at logMAR 0.3 at 6 months and again at 2 years; however, at 3 years, BCVA had deteriorated to logMAR 0.6 due to progressive enlargement of macular geographic atrophy beyond the area of image magnification. IMT position was stable (figure 1B) and corneal endothelial cell count reduced by 6% at 2 years, comparable with a standard anterior chamber lens.1
AMD is the most common cause of visual loss in adults >50 years in the developed world, affecting one-third of the >75 years population, typically bilaterally.2 3 Treatment is available for the neovascular form of AMD; however, therapies for dry AMD are currently limited.4 The proportion of AMD patients with significant visual loss (>6 lines of BCVA loss) increases with disease duration and development of end-stage features including geographic atrophy and subretinal scarring.4 AMD, particularly bilateral advanced disease, has a negative effect on quality of life (QOL) with better QOL outcomes when low vision aid training is instituted.5
Low vision devices (eg, handheld magnifiers) have long been the mainstay of treatment in advanced AMD but may be limited by musculoskeletal comorbidity.6 Novel intraocular magnifiers are now available as an adjunct to cataract surgery.7 The IMT (by Dr Isaac Lipshitz) is a miniaturised Galilean telescope which magnifies image size on the macula by ×2.7, engaging viable retina surrounding a central scar/atrophy providing BCVA gain of ≥2 lines in 90% when implanted in the better-seeing eye.7 Data from FDA studies and our own work show long-term preservation of corneal endothelial cell count comparable with traditional anterior chamber intraocular lenses.1 7 Clinical examination and imaging of the macula are possible through the IMT (figures 1C and 2A–C), enabling monitoring for progression and treatment of reactivated neovascular AMD. Visualisation of the far peripheral retina is limited; thus, peripheral retinal pathology or high myopia are contraindications for intraocular magnifiers. Though not treating the primary pathology of AMD, intraocular magnifiers, like the IMT, are useful functional adjuncts when medical therapy fails to maintain adequate vision. Though improvement in VA is not always sustained in the long term, the temporary delay in further deterioration positively influences visual QoL and is a useful consideration in this elderly population.

{kind=link}
{kind=link}
Optical coherence tomography (OCT) (Cirrus 5000, Carl Zeiss Meditec, Dublin, California, USA) images showing (A) en face view of retina extending to the arcades, (B) macular view OCT B-scan, highlighting geographic outer retinal atrophy and (C) wide field OCT B-scan.
Learning points
The implantable miniature telescope (IMT) may provide functional benefit in advanced age-related macular degeneration (AMD) (though not a return to driving vision) with good safety parameters in appropriate patients (ie, no peripheral retinal pathology, motivated to participate in visual rehabilitation training).
Careful preoperative assessment of benefit and safety should be performed with both anatomical measurements (ie, anterior chamber depth, axial length, endothelial cell count) and proprietary external telescope simulator, which illustrates magnification, field of vision and contrast to be expected via the IMT.
Retinal examination and imaging can be readily performed through the IMT device for AMD monitoring and treatment. While colour photographs are hampered by glare/artefact, Zeiss Cirrus 5000 optical coherence tomography images can be successfully acquired via the high-definition raster mode with line spacing 0.1–0.25 mm (ie, tightly packed), line length 3–6 mm, scan angle 0°, and any eye-tracking features deactivated.
Ethics statements
Acknowledgments
VisionCare Ophthalmic Technologies (Samsara Vision)
Footnotes
Contributors KAJS: patient care, manuscript drafting and revision. GM: patient care, manuscript drafting and revision. EA: device design, manuscript drafting and revision. DJK: patient care, manuscript drafting and revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests KAJS: none. GM: none. DJK: none. EA: device design, employee of VisionCare Ophthalmic Technologies.
Provenance and peer review Not commissioned; externally peer reviewed.