Article Text

Statistics from Altmetric.com
Description
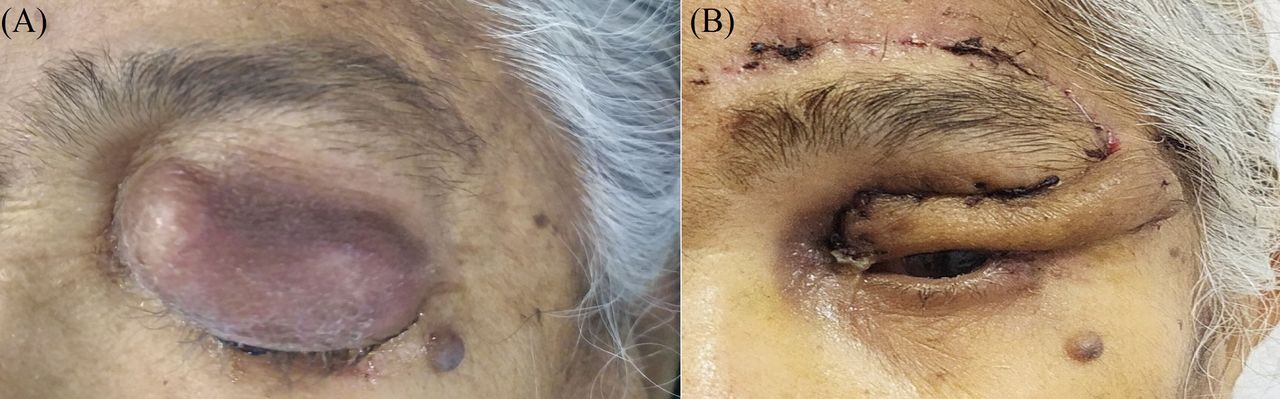
A 70-year-old Asian woman presented with a rapidly growing swelling in her left eyelid for the last month. It was associated with multiple bouts of spontaneous bleeding which resolved on the application of pressure. Clinical examination revealed a rapidly growing, violaceous mass lesion associated with soft-tissue ulceration and destruction of the tarsal plate (figure 1A). The mass effect resulted in ptosis of the upper eyelid. However, the vision was preserved in her left eye. The mass was painful and extremely friable. The contrast-enhanced computed tomography scan of the head and neck region did not show any lymphadenopathy. Fine-needle aspiration cytology of the swelling suggested either an appendageal tumour or a non-Hodgkin’s lymphoma. She underwent a wide local excision (WLE) with circumferential 5 mm margins to ascertain the definitive diagnosis and to control bleeding. The surgical defect was reconstructed via Fricke flap—a temporally based monopedicle forehead transposition flap. The postoperative period was uneventful (figure 1B). Histological analysis (figure 2A) revealed tumour cells arranged in an organoid pattern, cords, islands and sheets with brisk mitosis (4–5/HPF). On immunohistochemistry, tumour cells showed CD56 and chromogranin positivity with focal positivity for synaptophysin (figure 2B). A Ki-67 labelling index of 80% was noted. The distance from the closest margin was 3 mm. She was diagnosed as Merkel cell carcinoma (MCC) of the left upper eyelid, stage IIA (pT2N0M0) as per AJCC eighth edition. She received adjuvant radiotherapy following a discussion in the institutional multidisciplinary tumour board. She is currently disease free after 10 months of follow-up and is satisfied with the aesthetic outcomes.

(A) Preoperative photograph showing the violaceous mass involving left upper eyelid. (B) Postoperative photograph following tumour resection and Fricke flap reconstruction.

{kind=link}
{kind=link}
(A) Photomicrograph showing small to intermediate-sized tumour cells arranged in trabeculae with an occasional rosette-like arrangement, with fine salt and pepper chromatin, nuclear moulding and brisk mitosis (H&E, ×40), (B) diffuse cytoplasmic positivity for synaptophysin (Immunohistochemistry,×40).
MCC is a rare and aggressive neuroendocrine malignancy with male preponderance and predilection for Caucasians than other ethnicities. An association with Merkel cell polyomavirus has been reported in 60%–80% of specimens, especially of the old and immunosuppressed patients.1 About 46%–48% of all carcinomas present in the head and neck region of which 5%–20% epicentre in the eyelids.2–4 The eyelid MCC typically affects the upper eyelids especially near its margin and is associated with madarosis, skin ulceration, and distortion of the normal architecture. The tumours are usually misdiagnosed as cysts, chalazia or basal cell carcinomas.5 WLE with 5 mm margins is considered as an adequate margin to control the primary tumour when located in the periocular region contrary to 2.5–3 cm margins, as is used for cutaneous MCC elsewhere on the body. This is essential to preserve the integrity of as many facial aesthetic sub-units as possible without any compromise on oncological outcomes.6 Moreover, large postresection defects also pose a reconstructive challenge. Due to the aggressive biology and its exquisite radiosensitivity, postoperative adjuvant radiation therapy is often considered.7 8
This case highlights the diagnosis of MCC in the ethnicity less likely to harbour the same. Early diagnosis with a high index of suspicion is of paramount importance especially in the face for best functional and aesthetic outcomes and to avoid any mutilating surgery like the orbital exenteration that can hamper the Quality of life of the patients.
Patient’s perspective
The past month has been one of the most traumatic experiences of my life. This rapidly growing mass in my eyelid with the bouts of bleeding used to give me a feeling that my doomsday was fast approaching. Even though my vision was normal but I scared that I would go blind soon. I felt, that some vessel in my brain had burst due to which I got these intermittent bouts of bleeding, despite being reassured by my treating doctor that there was no disease inside my skull. I had to undergo some procedure as a part of my work-up where the doctors used a big needle to poke into my eyelid. Though the team was very co-operative, yet the whole scenario in itself was scary. The doctor told me that this mass was some kind of tumour and because of these bleeding spells, they advised me surgery. The idea of having a tumour scared me even more. I just wished and prayed to the almighty. Luckily, my surgery was uneventful and the doctors could also preserve my eye. I wish this does not happen again to me or to anyone else.
Learning points
Merkel cell carcinoma is a rare eyelid tumour in Asian ethnicity.
The treatment plan should be finalised based on the shared decision with the patient and family members and the multidisciplinary tumour board.
Wide local excision with adequate tumour-free margins is the primary treatment.
Adjuvant radiotherapy is usually added to the treatment protocol considering the high biological aggressiveness of the tumour.
Ethics statements
Patient consent for publication
Footnotes
Twitter @DrPankajGarg
Contributors Conceptualisation: PKG and PK. Clinical management of the case: PK, DC, NK and PKG. Drafting of the manuscript: PK. Revisions of the manuscript: PKG, DC, NK. Approval of the final manuscript: PK, DC, NK and PKG.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.