Article Text

Statistics from Altmetric.com
Description
A 62-year-old female patient presented with left radial side wrist pain for the past 4 weeks. She denied any history of trauma. On physical examination, she had swelling and tenderness to palpation in the first dorsal compartment with a positive Finkelstein’s test. On ultrasound, the first extensor compartment revealed complete septation with a thickened retinaculum only embedding the extensor pollicis brevis (EPB) tendon (figure 1) associated with hypervascularity and small tendon sheath effusion (figure 2). The abductor pollicis longus (APL) tendon was unremarkable. The patient was diagnosed with type II de Quervain’s disease (DQD) and conservative management was pursued including non-steroidal anti-inflammatory drugs (NSAIDS) and physical therapy that resulted in significant clinical improvement.

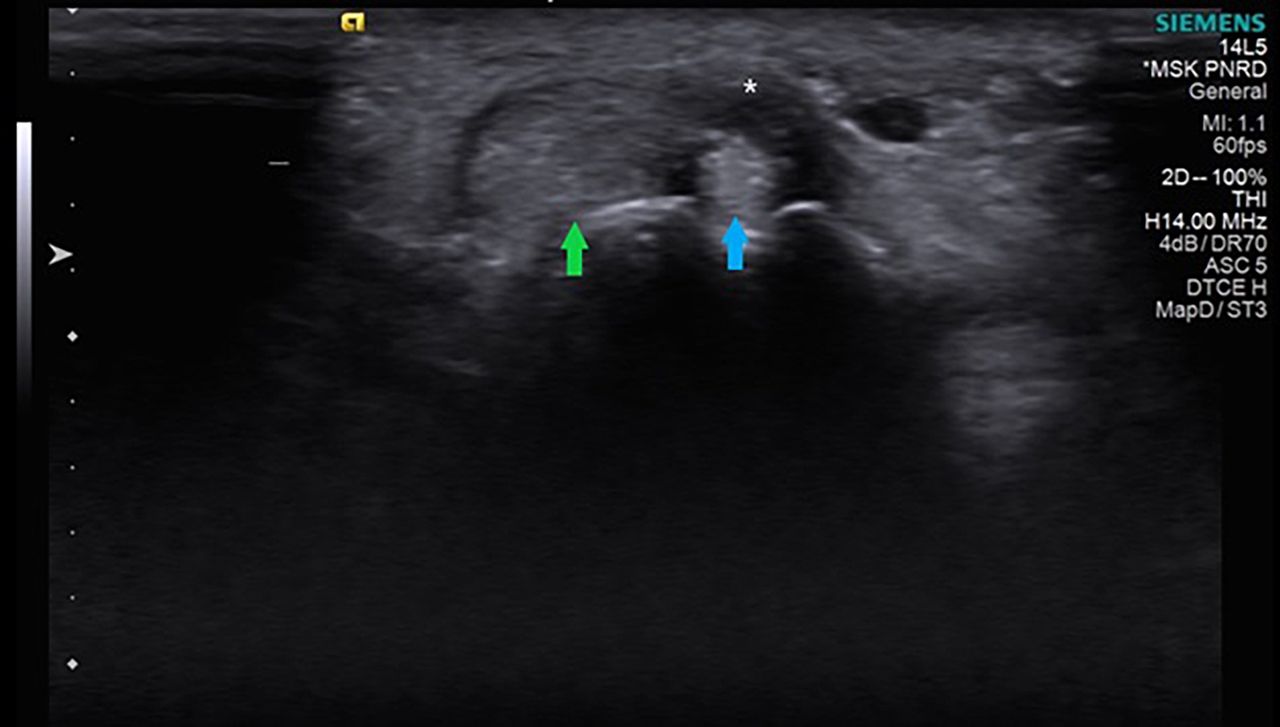
Axial view of the first compartment at the level of the radial styloid process, showing the thickened retinaculum (*) embedding only the extensor pollicis brevis (blue arrow). The abductor pollicis longus (green arrow) is unremarkable.

{kind=link}
{kind=link}
Axial view of the first compartment at the level of the radial styloid process, showing hypervascularity of the thickened retinaculum (*) embedding only the extensor pollicis brevis (blue arrow).
DQD is a stenosing tenosynovitis of the APL and EPB tendons in the first extensor compartment of the wrist.1 Metaplastic changes increase the thickness of the extensor retinaculum of the first compartment and reduce its cross-sectional area causing impingement of the APL and EPB. Instead of an inflammatory aetiology, a degenerative mechanism has been proposed after the observation of myxoid degeneration of the APL and EPB tendon sheaths in biopsies of DQD patients.2 Indeed, a case–control study found that a thickened retinaculum was found in all DQD patients and that inflammatory involvement of tendons was an inconstant feature.3
Although there are many non-modifiable factors (such as older age, female gender and anatomic variations) that contribute to DQD, modifiable (work-related) factors have not been recognised as risk factors.3 Indeed, a systematic review and meta-analysis concluded there was no causal relationship between occupational risk factors and DQD.4 Still, it is plausible that work-related activity may aggravate the wrist pain in DQD patients or in those predisposed to develop DQD.
The most common pattern is one or two APLs and one EPB in a single compartment,5 6 but several anatomic variations in the number of tendons and division pattern of this compartment have been described. Indeed, four types were classified by Hiranuma et al7: (type 1) APL and EPB share the same sheath; (type 2) complete septation, APL and EPB have separate tendon sheaths; (type 3) incomplete septation, APL and EPB have separate tendon sheaths only in the distal portion and (type 4) EPB-lacking type, tendon sheath is normal but lacks EPB.
When subcompartmentalisation is present in patients with DQD, the EPB is frequently more affected than the APL.5 The efficacy of steroid injections is dependent on its correct administration within the pathological subcompartment.5 Likewise, surgical treatment can be ineffective if the tendon sheath of the pathologic subcompartiment remains unreleased.3 5 8
This case should arouse awareness regarding subcompartmentalisation of the first extensor compartment of the wrist and how it can influence DQD treatment.
Learning points
Ultrasound is a useful imaging technique for diagnosing de Quervain’s disease.
Ultrasound provides important information about anatomic variations within the first extensor compartment.
Subcompartmentalisation should be detected as it allows proper steroid injection or surgical planning.
Ethics statements
Footnotes
Contributors RPD identified, managed the case and took the lead in writing the manuscript. JJ provided critical feedback and helped shape the analysis and review of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.