Article Text

Statistics from Altmetric.com
Description
A 69-year-old man with known chronic obstructive pulmonary disease (COPD) and extensive emphysema was investigated for potential treatment with endobronchial valves insertion. For this reason, a high-resolution CT (HRCT) was requested for the assessment of the emphysema distribution and fissures integrity. There was a recent history of spontaneous right pneumothorax treated successfully with chest drain placement. No CT scan was performed following the complete resolution of the pneumothorax as the patient was asymptomatic and the chest tube insertion was thought to be uncomplicated. The new HRCT investigating the potential treatment with endobronchial valves insertion was obtained and compared with previous imaging performed before the spontaneous pneumothorax. Over the intervening period, physical examination revealed progressive shortness of breath. The latest HRCT showed incomplete rotation of the right hilar structures. The right upper lobe was displaced inferiorly and laterally and the right lower lobe was displaced superiorly and clearly differed to the prior CT (figures 1 and 2). The degree of rotation was <90°. Although this was an unenhanced study, there were no CT features of infarction or necrosis with no obvious hilar vessels kinking suggestive of compromise of the arterial blood supply and venous-lymphatic drainage. The patient was treated with surgical reposition preventing further rotation of the hilar vessels and infarction and relieving his progressive symptoms.
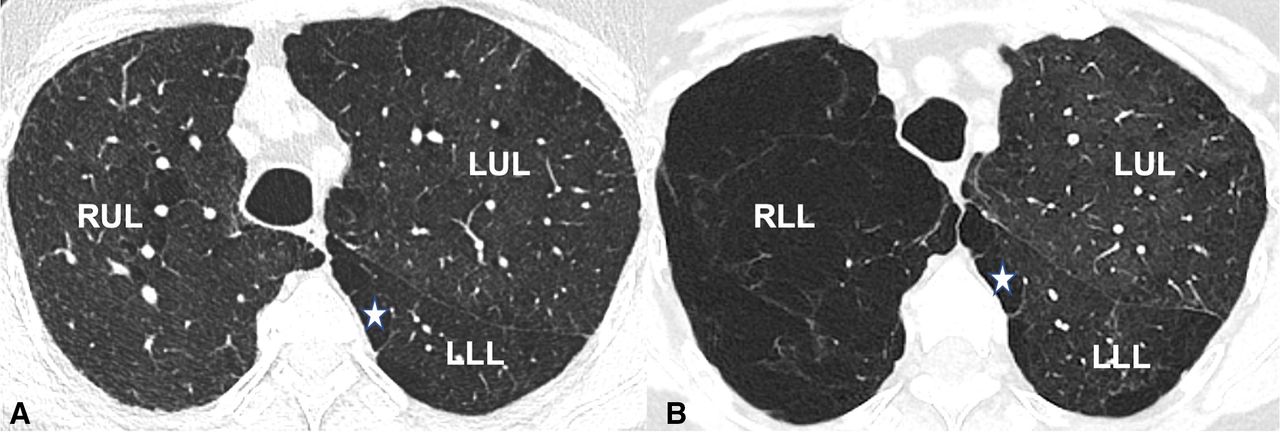
(A) Axial CT image shows the normal lobar anatomy with mild emphysematous changes in the right upper lobe. (B). CT findings 3 months later following the spontaneous pneumothorax and reinflation. Axial CT image at the same level demonstrates extensive emphysema in the upper lung zone which corresponds to the displaced right lower lobe. Pulmonary blebs (asterisk) in the apical segment of the left lower lobe demonstrating the same anatomical level. RUL, right upper lobe; RLL, right lower lobe; LUL, left upper lobe; LLL, left lower lobe.

{kind=link}
{kind=link}
(A) Coronal CT image shows the normal lobar anatomy demonstrating the origin of the right upper lobe bronchus (arrow). (B). Following the spontaneous pneumothorax, coronal CT image shows the abnormal lobar orientation of the right upper and lower lobe. It also demonstrates the downward orientation of the right upper lobe bronchus (arrow). (C). Sagittal CT image show the normal lobar anatomy of the right upper and lower lobe. Curved arrows show the anticlockwise rotation of the lobes. (D). Following the spontaneous pneumothorax, sagittal CT image shows the new positioning of the right upper and lower lobe. LLL, left lower lobe; LUL, left upper lobe; RLL, right lower lobe; RUL, right upper lobe.
Lung torsion is a very rare but life-threatening event, with a reported incidence of approximately 0.1%–0.4%.1 2 It is defined as the parenchymal rotation on the bronchovascular pedicle, accompanied by resultant airway obstruction and vascular compromise. It can occur usually as a complication of thoracic surgery, after large-volume thoracentesis and following traumatic pneumothorax.3–5 The clinical presentation depends on the degree of rotation. Acute, total lung torsion often presents with abrupt onset of chest pain and hypoxia. However, subacute, partial lung torsion is usually has a non-specific presentation and may be clinically occult or asymptomatic.4 The non-specific clinical manifestation leads to misdiagnosis up to 40% of the cases.6
Imaging plays a significant role in the detection of lung torsion. Chest radiograph is not specific with worsening consolidation and collapse while CT shows the abnormal lobar orientation, unusual fissure configuration and the degree of rotation of the hilar structures.4 CT angiography with multiplanar reconstruction is necessary to visualise the swirling of the pulmonary vasculature and the degree of arterial blood supply and venous-lymphatic drainage compromise, and a high level of suspicion is needed given the potential subtlety of findings.
The surgical management of lung torsion is repositioning or resection of the tortuous ischaemic lobe.6 The decision for detorsion or lobectomy usually depends on the viability of the torted lung which is better appreciated after open thoracotomy.
Recognition of the early signs of torsion and distinguishing torsion from other potential causes are of critical importance. Delay in diagnosis can result in significant pulmonary haemorrhagical infarction, necrosis and subsequent systemic sepsis and shock.
Learning points
Lung torsion is rare but can be associated with high mortality, and radiological detection requires a high index of suspicion to achieve early diagnosis and expedite life-saving surgical treatment.
CT is the gold-standard imaging tool and is critical for detection and assessing the degree of rotation and orientation of the pulmonary lobes.
Ethics statements
Patient consent for publication
Footnotes
Contributors Identified the case: KS. Conception and design: KS, EK and GTY. Literature search: KS. Drafting the manuscript: KS and EK. Revising the manuscript critically for important intellectual content: KS, EK and GTY. Final approval of the version to be published: KS, EK and GTY.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.