Article Text

Statistics from Altmetric.com
Description
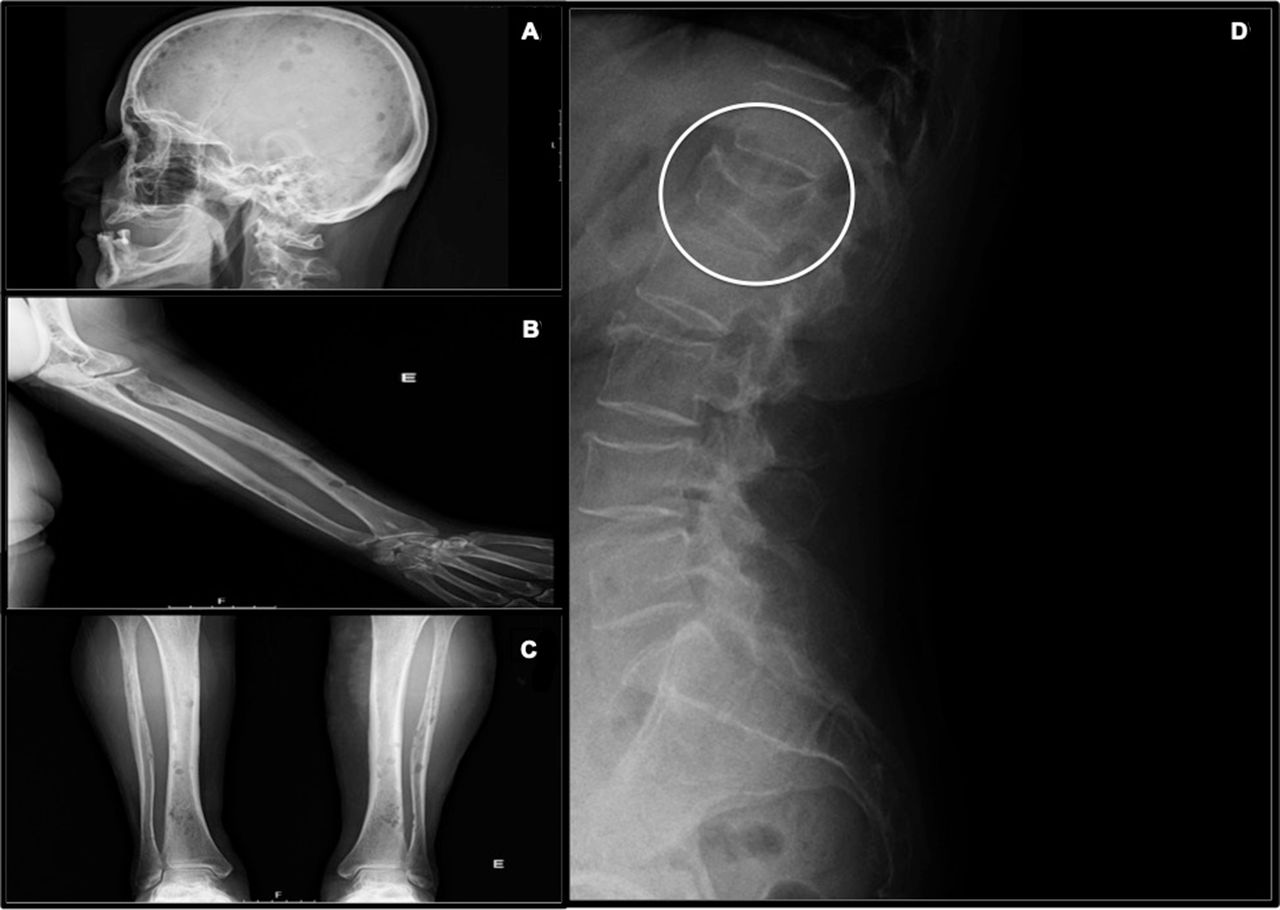
Multiple myeloma (MM) can present courses with lytic bone destruction caused by increased osteoclastic activity. These images are of a 64-year-old woman who presented to health services with neck and shoulder pain, anorexia, asthenia and weight loss, with months of evolution and multiple recurrences. She denied other symptoms. The radiological study showed lytic lesions of the cranial cap, tibia, fibula, radius, ulna and cervical region, suggestive of MM (figure 1). The diagnosis was confirmed by protein electrophoresis and light urinary chain dosage. The obtained radiography images are of particular interest given the lesser frequency of use of radiography as a complementary diagnostic method to CT examination, despite their value in guiding diagnosis.

{kind=link}
Lytic lesions observed in X-ray image of skull bone (A), left arm (B), lower limbs (C) and vertebral column with vertebra flattening as it is shown inside the circle (D).
MM is a malignancy of plasma cells that can cause the failure of the bone marrow, leading to anaemia, immune paresis with resultant infection, bone pain and fractures, high calcium levels and renal failure.1 MM is the second most common haematological malignancy, representing 10%–15% of all new diagnoses.2 The disease is more common in men, and the median survival is currently 4–8 years, partly depending on age at presentation.1 MM often presents with a high symptomatic burden, most commonly with fatigue and bone pain.3 The ability of haematopoietic stem cells to produce new blood cells is diminished, as the bone marrow becomes filled with malignant plasma cells, leading to anaemia and in some cases, but less commonly, thrombocytopenia and neutropaenia.4 The hallmark of MM is a severe destructive bone disease. Lytic skeletal lesions are also detected in approximately 80% of patients.4 The primary cause of the bone disease is increased osteoclastic activity, which occurs close to active myeloma cells. Other common findings are hypercalcaemia, impairment of renal function and infection.5
This image is of clinical interest as it evidences that a basic and quick approach bone X-ray examination allows for a relevant diagnosis. It is important to note that although 80% of patients with MM have lytic lesions, contrary to what was seen in this patient, many of these patients may be asymptomatic due to the bone lesions. If this were the case, and these images or a subset of them were obtained for another reason, the pattern present in the images would still point to a probable diagnosis of MM, which should be confirmed or ruled out by blood tests.
Learning points
For further guiding the diagnosis, radiography is a relevant complementary diagnostic test to perform as a first approach on patients with reports of bone pain and suspicion of multiple myeloma.
As radiography is a commonly requested test, it is important to be aware of certain changes that may indicate an additional diagnosis, even if it may be a finding in some circumstances.
Ethics statements
Patient consent for publication
Footnotes
Contributors OP: Conception and design of the article, acquisition of the data, drafting the article and revising it critically for important intellectual content, and final approval of the article. AAO, JM and MJR: Revision for important intellectual content and final approval of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer-reviewed.