Article Text

Statistics from Altmetric.com
Description
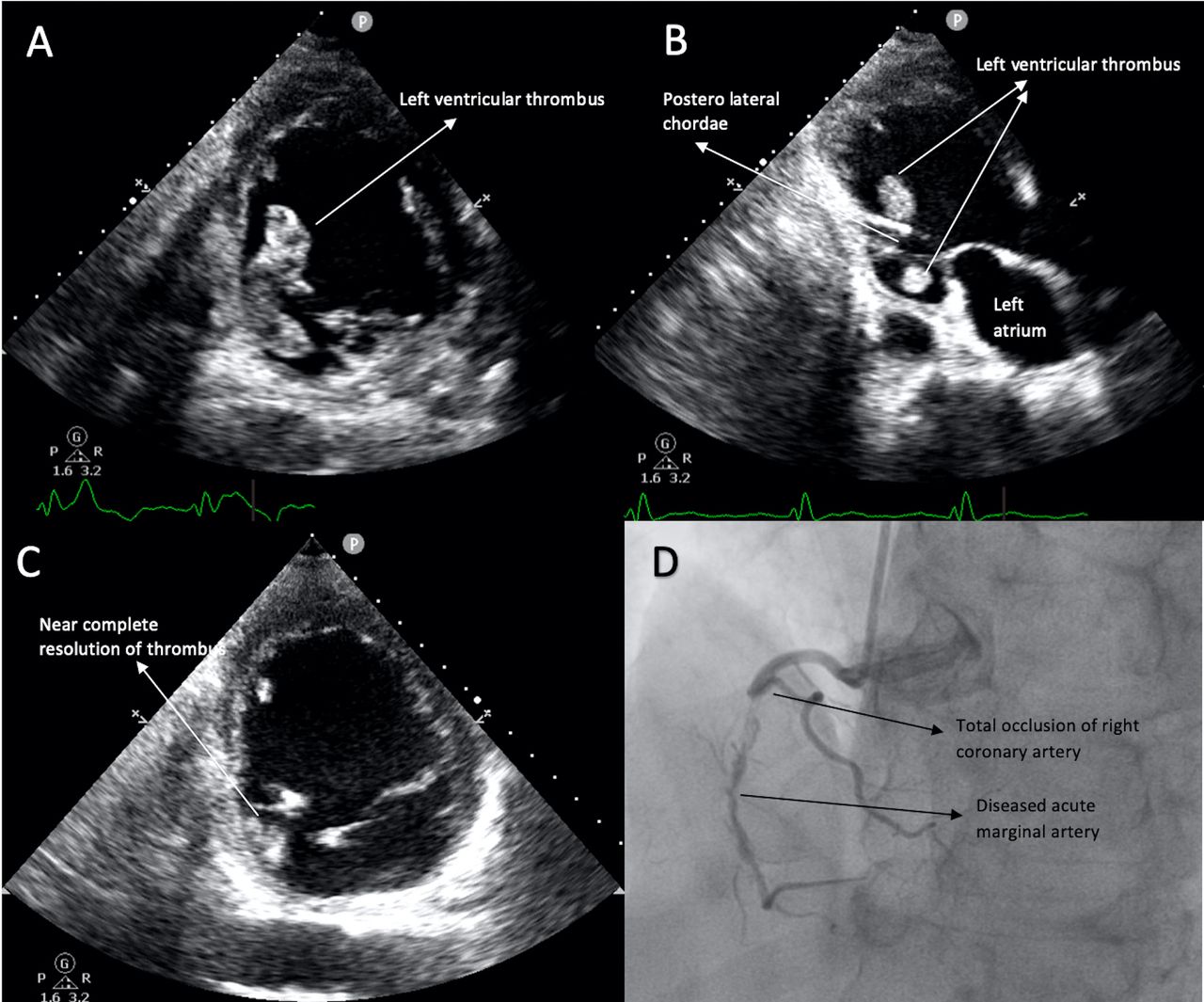
A 65-year-old man with a history of diabetes mellitus for the past 10 years presented with problems of dyspnoea on exertion New York Heart Association class II for 4 years, which worsened to class III–IV since last 1 week. He did not have any history of previous acute coronary syndrome or angina on exertion. ECG showed broad QRS complexes with interventricular conduction defect. Echocardiography showed severe left ventricular dysfunction with akinesia of inferior wall. There was a large mobile, protruding, dumbbell shaped thrombus in the left ventricle, which was attached to the inferior wall extending on both sides of the chordae of postero-medial papillary muscle (figure 1A,B; video 1). Coronary angiogram showed total occlusion of right coronary and mild disease in the left anterior descending artery. Patient was managed with enoxaparin and guideline directed medical therapy for heart failure. Repeat echocardiography done after 1 week prior to discharge showed near complete resolution of the thrombus (figure 1C). Patient did not develop any thromboembolic manifestations. Patient was discharged on warfarin, with a plan to continue the same for 6 months.
{kind=link}
(A) Transthoracic echocardiography in parasternal short axis view showing thrombus in the left ventricle. (B) Transthoracic echocardiography in parasternal long axis view showing thrombus in either side of the posterior chordae. (C) Repeat echocardiography showing near complete resolution of the thrombus. (D) Right coronary artery angiogram showing complete occlusion and diffusely disease acute marginal branch.
Left ventricular clot in ischaemic cardiomyopathy is frequently seen at the apex and the anterior wall. Clot in the septal wall is seen in 11% and its occurrence in the inferior wall is very rare comprising of only 3% cases with ischaemic cardiomyopathy having ventricular thrombus.1 The incidence of left ventricular clot postmyocardial infraction in the current reperfusion era is around 5%.2 The risk factors for development of left ventricular clot include anterior wall myocardial infarction, especially involving proximal left anterior coronary artery, severe left ventricular dysfunction (ejection fraction <30%).3 Presence of significant mitral regurgitation might be protective against clot formation, as the enhanced early diastolic flow into the left ventricle prevents stasis.4 Mobile and protruding clots have a greater tendency for embolisation. Larger clots, thrombus with echo-lucency and thrombus located close to hypercontractile myocardium also have higher chances of embolisation.4 Majority of the clots embolise within the first 4 months.5 The management of left ventricular thrombus is still controversial. Anticoagulation remains the mainstay of therapy, either heparin or warfarin. Thrombolysis and surgical removal of clot were done previously, but not practised anymore. Novel Oral Anticoagulants (NOACs) are not extensively studied in this patient population. Of late there are reports of such patients being successfully treated with NOACs.6 Although there are not much data on the optimal duration of therapy, it is a routine practise to give anticoagulants for 3–6 months as the embolic risk is higher in the initial few months.
Learning points
Left ventricular clot is commonly seen in the apex or the anterior wall.
Thrombus located in the inferior wall of left ventricle is very rare.
Mobile and protruding clots possess high risk of embolisation.
Warfarin for 3–6 months is the mainstay of therapy for left ventricular clots.
Footnotes
Contributors ASA was involved in conceptualisation, patient care, data collection and in writing the manuscript. SG was involved in patient care and proofreading the manuscript. HSI provided critical inputs to the manuscript. SK was involved in writing the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.