Article Text

Statistics from Altmetric.com
Description
In the maxillofacial region, foreign bodies occur due to trauma or therapeutic interventions.1 One of the most commonly reported foreign bodies in the jaw bones are filling materials.2 Ghafoor et al described a rare case in which a wide area of bone loss with loss of two teeth was related to an intra-osseous foreign body reaction due to amalgam displacement in the extraction socket.3 Another clinical case by Fredrik et al illustrated calcium hydroxide paste displacement into the mandible and the advantages of retrieving such displaced material before symptoms worsen.4 Multiple imaging techniques can be used to localise the foreign bodies which include plain radiographs, CT, MRI or ultrasound.5 This case clearly demonstrates an iatrogenic cause for discomfort and irritation of the mandible due to a displaced composite restoration fragment requiring surgical referral and treatment, which was potentially avoidable.
A 25-year-old male patient presented with a complaint of discomfort in the left mandible since last 6 months. On inspection, the area of discomfort was localised in the region of teeth #36 and #37. There was mild erythema and swelling in the region. There was no facial swelling, cervical lymphadenopathy or trismus on physical examination. Intra-oral examination did not reveal tenderness, pus discharge, bleeding or any other secondary symptoms. A composite restoration was noticed on tooth #37. The patient had a history of surgical removal of tooth #38 6 months prior. Panoramic radiograph did not show any significant findings. The patient was advised to maintain good oral hygiene and gargle with saltwater three times per day for 2 weeks. A review was scheduled after 2 weeks during which the patient did not report any change in the symptoms. A Cone Beam Computed Tomography (CBCT) was advised, which revealed a small radio-opaque area in the gingival soft tissue overlying in the alveolus lateral to teeth #36 and #37 (figure 1).
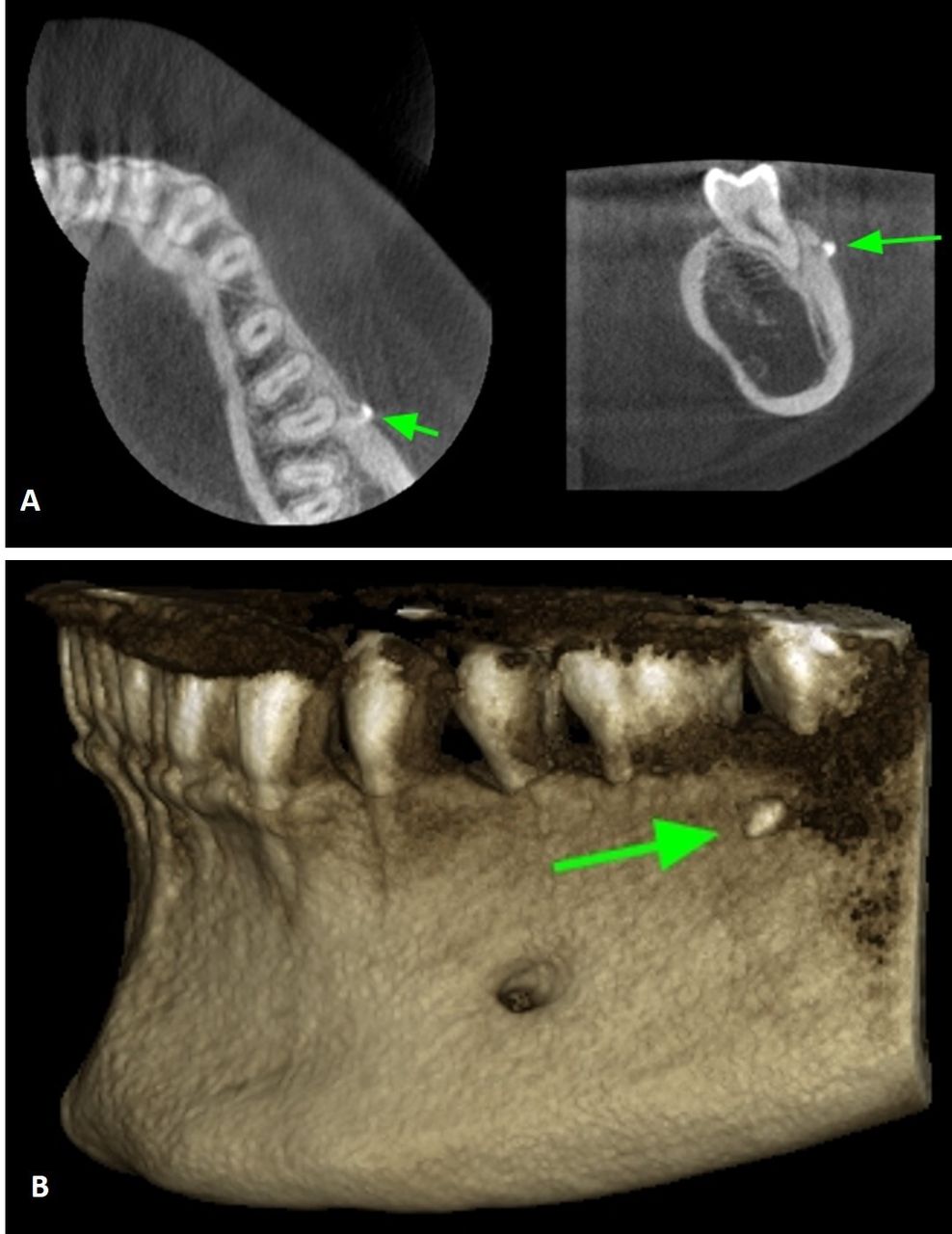
(A) Cone Beam Computed Tomography (CBCT) of the patient, green arrow pointing to the foreign body between teeth #36 and #37. (B) Three-dimensional (3D) CT of the patient, green arrow pointing to the foreign body between teeth #36 and #37 (scale 1.43) Planmeca 3Ds CBCT unit (Helsinki, Finland); 200 μm voxel, 90 kvP, 12 mA, 12.35 s exposure.
The patient was prepared, and surgical retrieval of the foreign body was performed after taking a thorough medical history. An inferior alveolar nerve block was administered using 2% lidocaine with 1:100 000 epinephrine. A modified wards incision was placed, and the flap was carefully reflected, not to displace the foreign body. A white coloured material was observed after careful exploration in between teeth #36 and #37 (figure 2). The material was seen to be embedded between the periosteal layer and the bone. The foreign body was then removed cautiously, and the site was irrigated well with saline. The flap was secured with simple interrupted sutures using (3-0) silk. On careful inspection of the adjacent area, it was found that a small piece of the composite restoration had chipped off from the distal most aspect of the tooth #37 and had displaced into the gingival soft tissue overlying the mandible, which in turn caused the irritation. The patient when reviewed 2 weeks postoperatively was asymptomatic.

{kind=link}
{kind=link}
The retrieved composite particle from the mandible is encircled.
Learning points
Dentists should be mindful of restorations on teeth adjacent to surgical site.
In case of any doubt of dislodged fragments of restoration, attempts should be made to recover them from the tissues.
Most displaced foreign bodies in mandible are found only during imaging or when patients complain of symptoms.
Ethics statements
Patient consent for publication
Footnotes
Contributors AMG contributed to patient treatment, conception and design. AKA contributed to drafting the work and revising it critically for important intellectual content. AnM contributed to defining intelectual content, design, literature review and manuscript editing. ArM contributed to literature review and manuscript editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.