Article Text

Abstract
This is a case of a 54-year-old woman managed as a case of osteogenesis imperfecta type 1 who sustained a left subtrochanteric fracture and eventual ankylosis of both hips after surgery and immobilisation. These injuries rendered her bedridden, maximally assisted in transitions and transfers, and unable to be positioned past 30° of backrest elevation. The patient underwent a bilateral Girdlestone procedure and had tailored progressive postoperative rehabilitation in both the inpatient and outpatient settings. The patient also continued to receive bisphosphonates during her preoperative and postoperative period, to improve bone stock and aid in relieving pain. Through the efforts of a team of physiatrists, geneticists and orthopaedic surgeons, the patient was able to achieve pain-free sitting, independent transitions and short-distance ambulation, which have allowed her to care for herself more effectively and return to her work and activities of daily living.
- rehabilitation medicine
- orthopaedics
- genetics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Osteogenesis imperfecta (OI) is a highly heterogenous disorder characterised by bone fragility. Prognoses may vary depending on the type of OI, and much of the literature on OI in adults have been viewed through the lens of genotypic and phenotypic correlations.1 With the advent of bisphosphonate therapy, recent studies have also highlighted its value in improving OI outcomes.2 Rehabilitation care, although recognised as important, has been explored more extensively on its effects in children than in adults.3
The Girdlestone resection arthroplasty was first described by Gathorne Robert Girdlestone in 1928 as a technique to treat tuberculosis and other disorders of the hip wherein no formal articulation between the pelvis and femur is established after resection of the femoral head.4 With the advent of replacement arthroplasty, the Girdlestone arthroplasty is considered as a procedure performed as a last resort in cases of significant infection, poor bone stock or failed total hip arthroplasty due to decreased functional outcomes.5 It has been documented in use for patients with neglected femoral neck fractures, failed osteosynthesis, failed hemiarthroplasty and painful aseptic osteonecrosis of the femoral head.6 Incidence of the procedure is generally low, with only 43 procedures performed from 1990 to 2002 in two large hospitals in the UK,7 with recent trends pointing that the conduct of the procedure today is even lower. There is also a noted lack of literature on the bilateral procedure and its outcomes, with only anecdotal evidence of three patients, who were eventually able to ambulate with gait aids.8 Its application on a patient with OI has not been described in the literature.
The purpose of this case report is to describe and document the functional outcomes of an adult with complex orthopaedic impairments after rehabilitation following bilateral Girdlestone procedure, who achieved ambulation with multidisciplinary collaboration.
Case presentation
Consent for this case report was explained and requested from the patient, which she gave under the condition to conceal her name and face.
The patient is a 54-year-old female accountant. She was born at full term to a then 34-year-old father and 26-year-old G2P1 mother. Immediate neonatal course was unremarkable. Developmentally, her milestones were at par with her sibling, but she was noted to be smaller than expected for her age. At the age of 3 years, the patient was noted to have bowed legs, prompting consult. She was managed as a case of rickets and underwent bracing of both knees, with eventual bilateral epiphyseal stapling at the age of 11 years. No similar condition was noted in the family. She was lost to follow-up thereafter.
At the age of 14 years, the patient slipped on the floor, breaking her right femur. On consult, she was then managed as a case of OI and underwent an open reduction internal fixation (ORIF) with plates and screws. She was eventually able to ambulate after a year, and continued follow-up with her local physician.
In 2012, at the age of 48 years, the patient tripped and sustained a left subtrochanteric femoral fracture, rendering her non-ambulatory. She again underwent an ORIF. In 2013, due to a fracture at the proximal site of attachment of her implanted plate, she underwent revision ORIF. At that time, the patient was still unable to sit and ambulate due to pain. She consulted with orthopaedics and rehabilitation medicine at the Philippine General Hospital (PGH) and underwent removal of her plates and screws in October 2014, with intraoperative findings of a healed femoral fracture. She was placed on a hip spica and sent home with modest pain improvement.
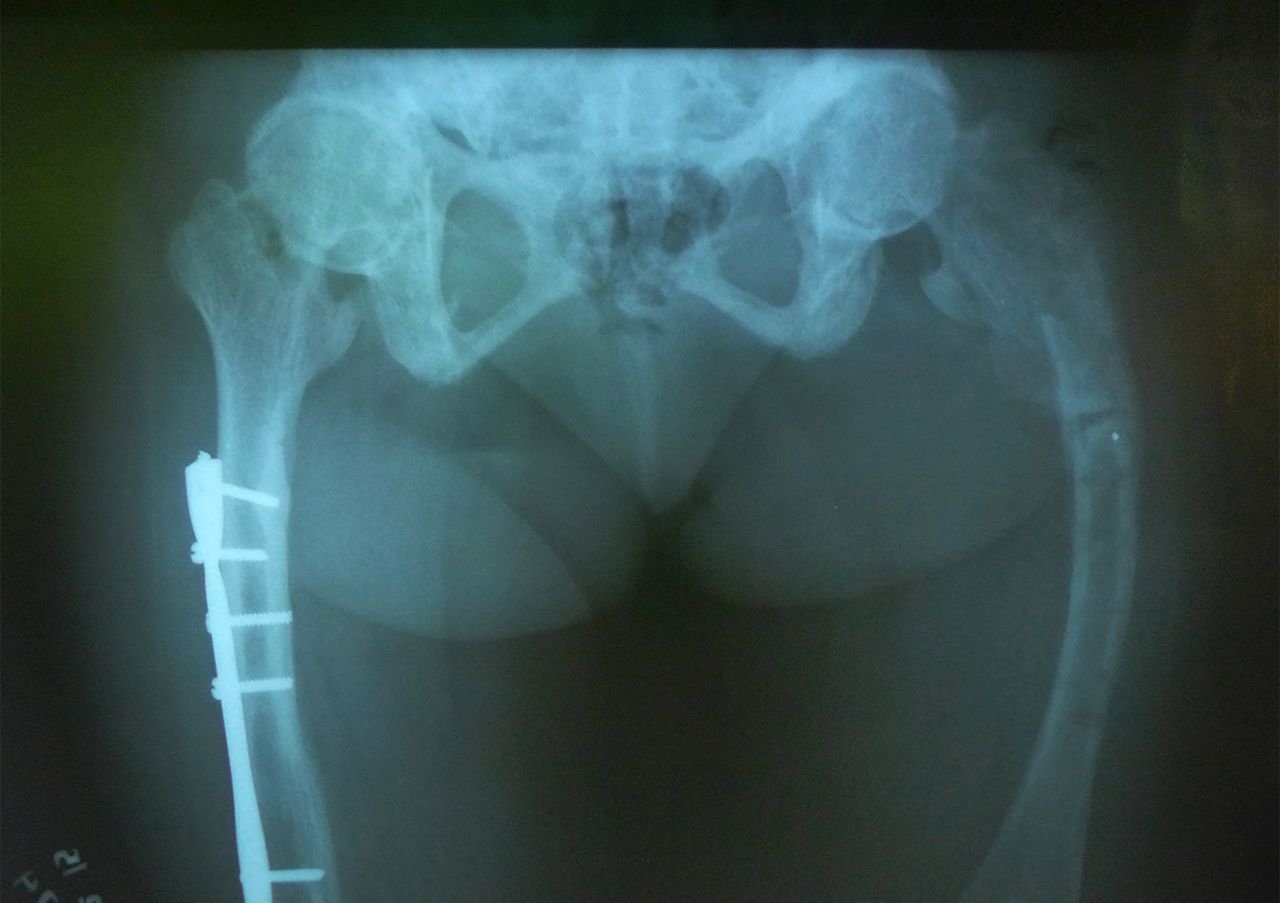
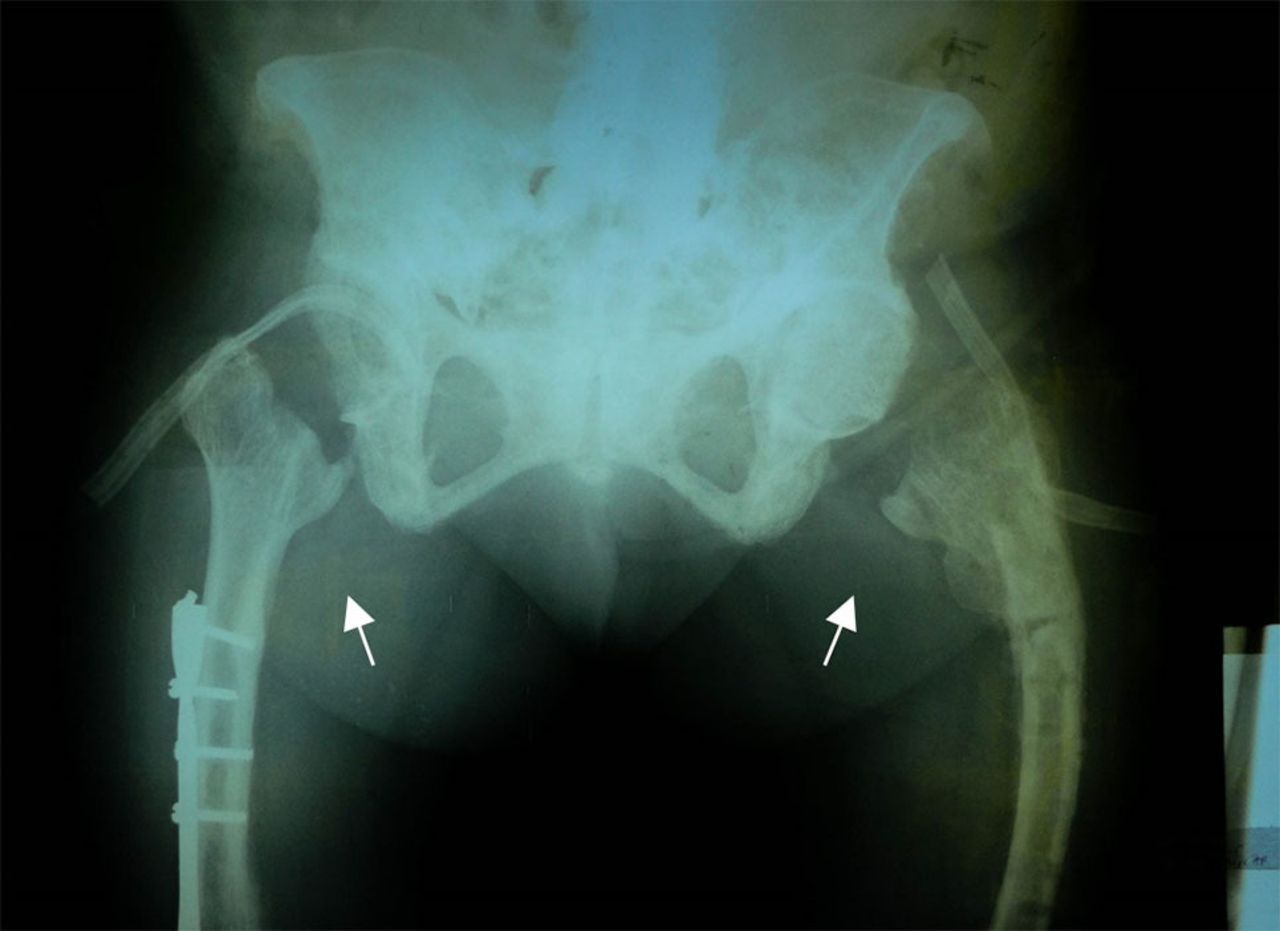
Prior to discharge and in the interim, the patient was managed by the genetics service, who clinically diagnosed the patient with OI type 1 and prescribed pamidronate infusions. On removal of the hip spica, there was noted limitation of the patient’s range of motion (ROM) of bilateral hips, only allowing low backrest elevation. Radiographical findings showed ankylosis of both hips (figure 1). She was readmitted in November 2015, and findings of preoperative examination showed passive hip flexion of 0°–30°, and 0°–12° of the right and left hips. There was also noted limitation of the patient’s cervical ROM on all planes, and that she was maintained in kyphosis of the neck. She underwent bilateral Girdlestone procedure during the admission (figure 2). To prevent postoperative complications and to facilitate functional recovery, the patient was then referred for inpatient rehabilitation and management.

Anteroposterior radiograph of the patient’s pelvis taken prior to Girdlestone arthroplasty.

Anteroposterior radiograph of the patient’s pelvis taken post-Girdlestone arthroplasty, with absence of the anatomic head and neck of both femurs (short arrows).
Treatment
At the time of referral, there was noted pain on movement of the lower extremities, with both legs placed in traction. At this time, rehabilitation goals included alleviation of pain and prevention of complications of immobility. The patient was prescribed icing and transcutaneous electrical nerve stimulation at the perioperative area and instructed on isometric exercises of the lower extremities.
Two weeks postprocedure, the traction was removed and the patient progressed to bed mobility exercises as well as assisted ROM exercises of bilateral lower extremities. She was eventually cleared for sitting, strengthening of bilateral hip flexors and out-of-bed exercises. Prior to discharge, she was able to tolerate wheelchair rides with the backrest at 90°. At this time, she was maximally assisted in transfers. She continued physical therapy at home and was able to continue ROM and conditioning exercises. She remained primarily bedbound and assisted in transfers to a bedside chair, as well as in performing activities of daily living requiring mobility, particularly toileting.
In May 2017, the patient was readmitted to PGH for progressive rehabilitation care in coordination with genetics service for her pamidronate infusions. She was then able to tolerate standing exercises for 2 min and gradually progressed to ambulation training with a standard walker during her month-long admission. She continued rehabilitation management on an outpatient basis. Therapy included ROM exercises, strengthening of bilateral crutch bearing muscles, standing balance and tolerance exercises, and short-distance gait retraining with an adult standard walker.
Outcome and follow-up
During the patient’s follow-up last August 2018, the patient was noted to have limited passive ROM of both hips, knees and ankles, particularly on hip extension and internal rotation as well as knee flexion (table 1). Given these impairments, the patient had achieved functional ROM with adequate strength to provide resistance.
Lower extremity passive range of motion findings 33 months postoperatively, with normal values20
The patient was able to complete the Timed Up and Go test, with an average time of 2 min and 11 s. Although this result classifies her under an increased risk of falls requiring standby assistance and a gait aid,9 the patient was able to finish the examination—a feat she was unable to perform 6 months prior.
The patient was also assessed using the modified Merle d’Aubigne-Postel score, the Harris hip score, the functional independence measure and the short form-36 (table 2). From these assessment tools, the patient showed improvements in her independence and her general hip function. Although the patient had lower scores in functional capacity and physical domains than others who had a unilateral Girdlestone or a combination unilateral Girdlestone-contralateral hip arthroplasty,10 the patient had similar ratings in the social and emotional domains, as well as in pain, vitality, mental health and overall status.
Description of assessment tools used and summary of findings
The patient also underwent motion analysis (figure 3). On assessment of her kinematics and temporospatial parameters (video 1), there was decreased walking speed and cadence, as well as an increase in the peak anterior pelvic tilt. There was also noted decreased peak hip extension, with decreased ankle plantar flexion during the third rocker. These findings are comparable with a local study performed with ambulatory OI patients, from type I to V.11

{kind=link}
{kind=link}
{kind=link}
Coronal (left) and sagittal (right) views of the patient undergoing motion analysis.
Disclaimer: this video summarises a scientific article published by BMJ Publishing Group Limited (BMJ). The content of this video has not been peer-reviewed and does not constitute medical advice. Any opinions expressed are solely those of the contributors. Viewers should be aware that professionals in the field may have different opinions. BMJ does not endorse any opinions expressed or recommendations discussed. Viewers should not use the content of the video as the basis for any medical treatment. BMJ disclaims all liability and responsibility arising from any reliance placed on the content.
Discussion
In the management of an adult with OI, it is important to keep in mind that, although fracture rates generally decline as a patient reaches skeletal maturity, the incidence of fracture in persons aged 20–54 years, and 55 years and above, is 6.2 and 4.1 times as high as those of the normal population, respectively.12 Prevention can be done with the administration of bisphosphonates, which increase bone mass density and reduce fracture risk.13 Decreased pain may also be an effect of bisphosphonate administration,14 which also facilitates therapy exercises. Once with a fracture requiring surgical intervention, factors, such as bony deformity, increased risk of fractures and shorter limbs, must be considered. Load-sharing intramedullary devices are strongly preferred over locking plates, as the latter can promote stress shielding and can lead to bony resorption. As was demonstrated by our patient, the ends of plates are also prone to fracture, as these are areas with a high concentration of stress.15
The congenital weakness in bones, ligaments and muscles in OI, and their accompanying skeletal deformities and functional limitations emphasises the importance of rehabilitation care in attaining independent living and active social participation. Active movement is encouraged to enhance musculoskeletal strength and cardiovascular fitness. Programmes are tailored according to the degree of motor development of the individual, clinical severity of OI and attained ability.16
After a fracture, guided rehabilitation care is even more necessary. Prolonged immobilisation is detrimental to recovery, as fracture risk may be further increased by disuse osteopenia, weakness and functional impairment.17 Current consensus is that the cycle of fracture, immobilisation, osteoporosis and refracture must be interrupted, as the possibility of autonomy is inversely correlated to subsequent injury and deformity, especially in later years.18
The Girdlestone arthroplasty has been progressively left aside in favour of replacement arthroplasty due to its functional inferiority, mainly attributed to poor postoperative joint stability and subsequent limb length discrepancy, eventually leading to increased energy expenditure and stance changes resulting to possible ambulation support.19 However, it still is able to provide some level of pain relief, improvement of patient function and an increase in patient satisfaction. In our patient, the orthopaedic service chose to proceed with this procedure with the primary aim of allowing the patient to sit.
Through the efforts of physiatrists, geneticists and orthopaedic surgeons, as well as the rehabilitation medicine team, the patient was able to achieve pain-free sitting, independent transitions and short-distance ambulation. These functional improvements have allowed the patient to care for herself more effectively and return to her work as a municipal accountant. The outcome measures give a quantitative scale to the patient’s improvement and provide guidance as to which areas need more focus.
Patient’s perspective
I am thankful to God, my support system, and my doctors from ortho, rehab and genetics for my continued progress. At the start, I was unsure of the surgery, especially since they were going to remove my hips. But now, I can stand and walk around on my own, even if just a little bit, for the first time in 6 years. I still need help with a lot of things, but I believe that with the help of the entire team, I can achieve even more.
Learning points
Well-structured therapeutic interventions and strong multidisciplinary collaboration are immensely important for patients with complex musculoskeletal concerns.
For cases such as these, preparation for and commitment to a prolonged rehabilitation course is necessary for continued improvement in functional ability.
Although not all impairments may be reverted to normal in complex orthopaedic cases, a significant level of functional improvement and enhancement of quality of life may be achieved.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to acknowledge the assistance of Dr Juanito S Javier, whose knowledge and expertise regarding the patient’s case proved invaluable to the report.
Footnotes
Correction notice The article has been corrected since it was published. The affiliations have been updated.
Contributors IS: Served as the primary investigator of this study, selected and administered functional tests, performed the technical analysis of the patient, reviewed the literature and wrote the manuscript. JEA: Supervised management of the patient and gave input during the examination period. She also edited and reviewed the final manuscript. MMLA: Gave critical information on the status of the patient and the nuances of her management, and assisted in editing the manuscript. CES: Assisted in the general design of the report, and gave feedback on the completed manuscript. All authors have read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer-reviewed.