Article Text

Statistics from Altmetric.com
Description
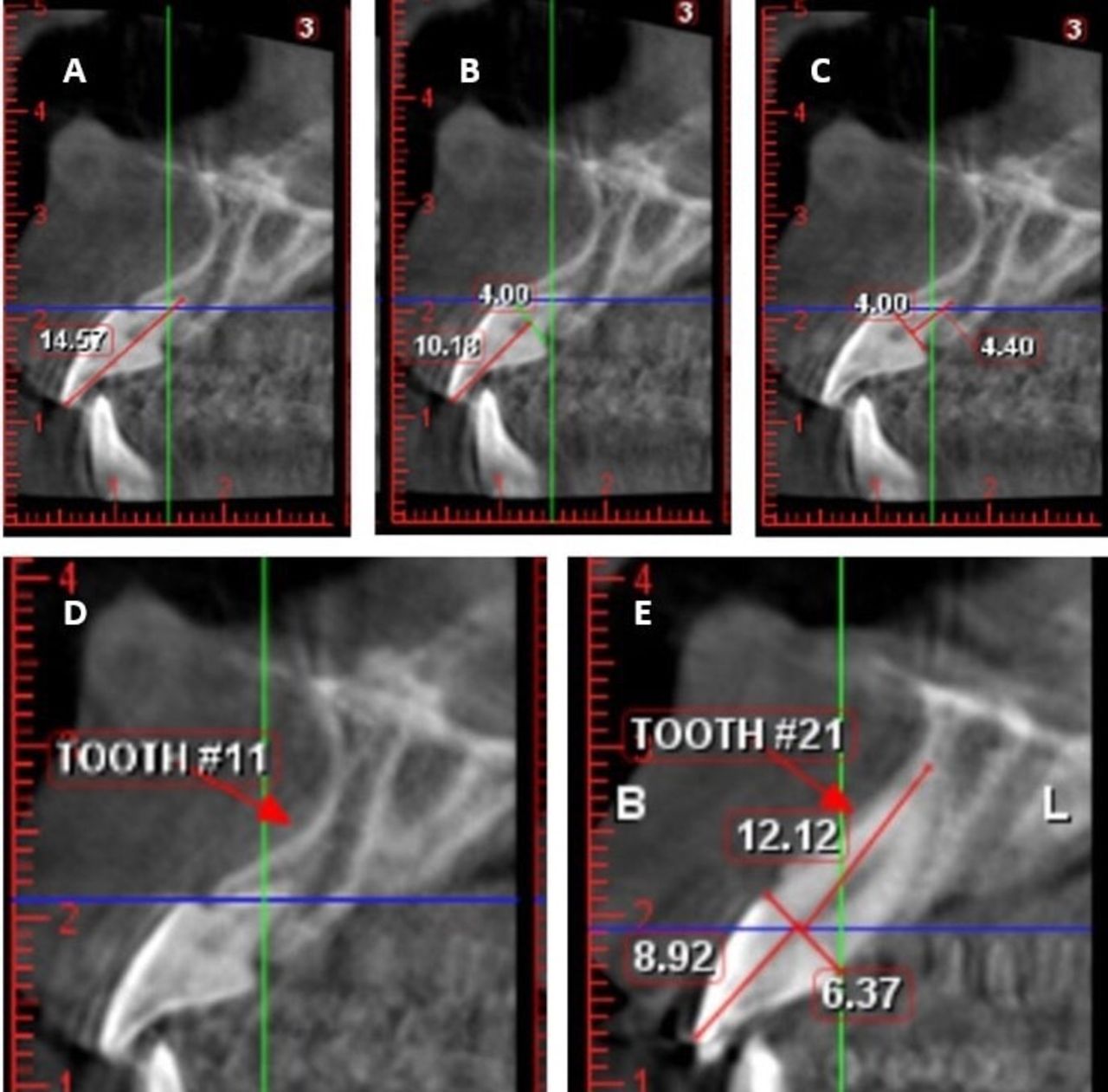
A 19-year old female patient with the report of irregularly placed upper front teeth sought orthodontic treatment. Clinically,she exhibited an edge to edge incisal relationship and class III malocclusion. Panoramic radiograph revealed the presence of all teeth including four unerupted third molars. Teeth 16, 26 and 36 were restored due to dental caries. The periodontal and supporting tissues were found to be healthy. Due to suspicion of dental caries on teeth 11 and 12, an intraoral periapical radiograph (IOPA) was taken, which showed abnormally short and conical root with respect to tooth 11, along with well-defined radiopacity on the distoproximal aspect of tooth 11 suggestive of previous restoration. Thereafter, a detailed radiological examination was carried out using cone beam CT (CBCT) in order evaluate the short-rooted tooth,1 2 sectional image obtained from the CBCT showed that total length of the tooth was 14.57 mm, crown length from incisal tip to cementoenamel junction (CEJ) was 10.18 mm and root length from CEJ to the tip of the root was 4.40 mm, (figure 1A–C). The labial alveolar bone concavity over tooth 11 appeared to be more pronounced as compared with the bone morphology of the adjacent tooth 21 (figure 1D,E). This finding suggests a possible developmental aetiology.

Cone beam CT image of (A) total length of tooth 11, (B) crown length of tooth 11, (C) root length of tooth 11, (D) labial alveolar bone morphology of tooth 11 and (E) labial alveolar bone morphology of tooth 21 with measurements.
On further evaluation, the patient stated no history of trauma or previous orthodontic treatment. Clinically, the crown of tooth 11 had the same size and morphology when compared with the unaffected tooth 21. This is in accordance with the literature on short root anomaly cases.3 The root is theoretically considered short when its crown–root ratio is more than 1:1.4 Tooth 11 did not exhibit any signs of mobility and tested positive for pulp sensibility. All these findings were suggestive of short root anomaly (SRA).
SRA is a rare condition that is often allied with genetic predisposition and higher female predilection.5–9 The aetiology of SRA is mostly characterised as idiopathic.10 Other suggested aetiologies include congenital or developmental origin,3 7 external influences like trauma,11 syndromes,12–14 chemotherapy and radiotherapy.15 Literature affirms that this condition always affects both the central incisors.4 On the contrary, the clinical report presented here displays a case of unilateral pattern of SRA. Additionally, the root length was considerably short in comparison to its bilateral counterpart. Based on the literature search, there is a dearth in reports exhibiting unilateral cases of SRA, which makes this report unique.
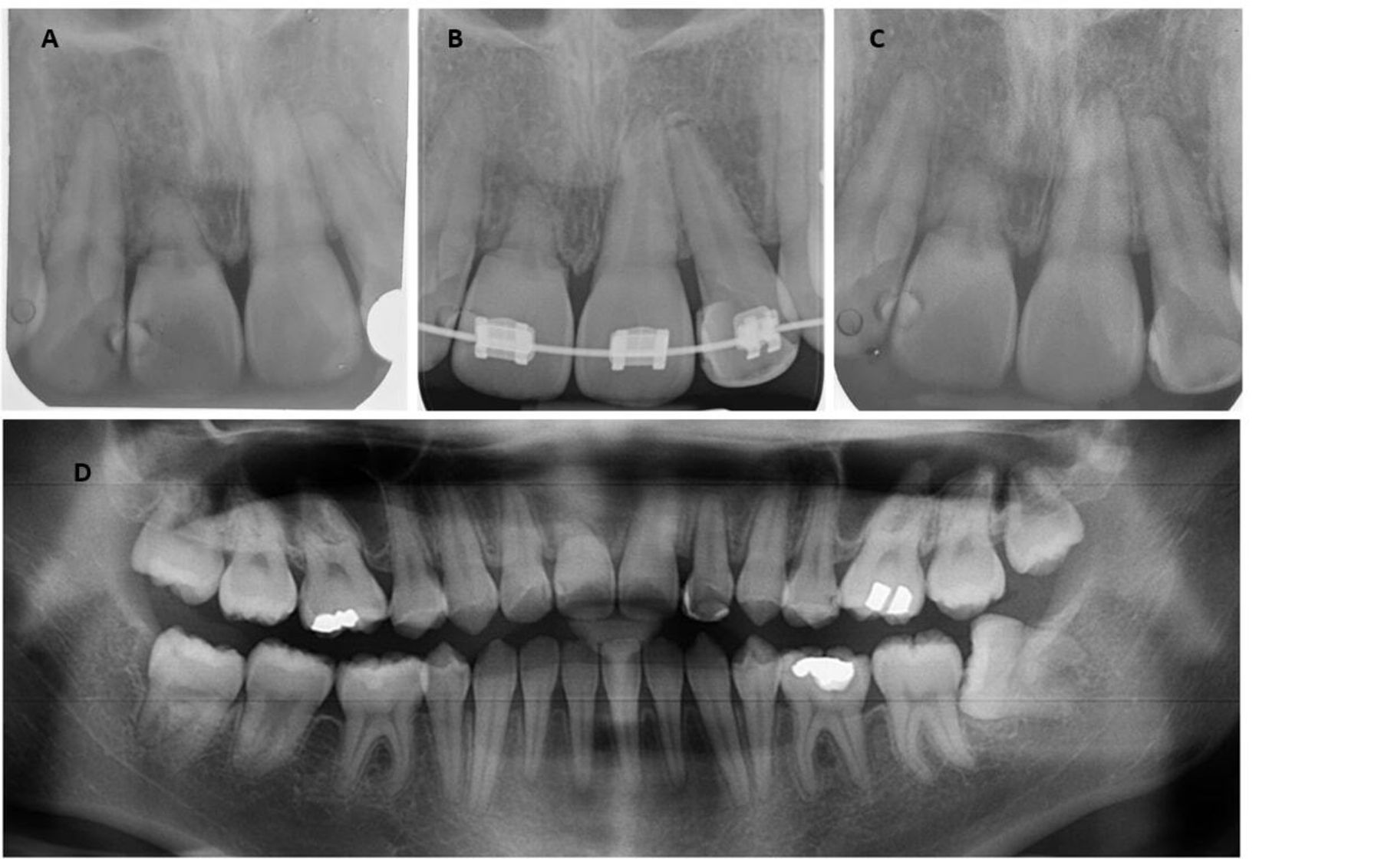
Orthodontic treatment was initiated since the tooth 11 was asymptomatic. However, light intermittent forces were employed to bring about tooth movement and to prevent deleterious effects on tooth 11.16–18 Prior to treatment onset, the patient was informed about the condition she presented with and the limitations, risks and objectives of treatment. After signing an informed consent form, orthodontic therapy was initiated. During the course of treatment, constant monitoring of root and bone tissue in relation to the tooth 11 with SRA was ensured.19 20 Orthodontic treatment was satisfactorily completed with sufficient overjet, overbite, incisor angulation and stable posterior occlusion. The posttreatment IOPA and panoramic radiograph revealed unaltered root morphology with adequate bone support, implying that orthodontic treatment is not an absolute contraindication in asymptomatic SRA5 15 21–23 (figure 2). The patient will be followed up over the next 5 years on a 6-month interval to monitor the prognosis of the tooth.

{kind=link}
{kind=link}
(A) Pretreatment IOPA, (B) during treatment IOPA, (C) posttreatment IOPA of tooth 11 and (D) posttreatment panoramic radiograph showing unaltered root and bone structure after orthodontic treatment. IOPA, intraoral periapical radiograph.
Patient’s perspective
I was unaware of this condition as I had never experienced any pain or distinct tooth movement involving my incisor. I am relieved to know that the tooth is stable and orthodontic therapy has improved the longevity of the tooth.
Learning points
Pretreatment orthodontic radiographs are extremely helpful in careful evaluation of the crown–root ratio of individual teeth in order to rule out iatrogenic root resorption.
Pretreatment radiographs can also be used as baseline or reference points to evaluate further reduction in root length due to resorption arising from inadvertent forces. Hence, periodic radiographs must be taken to monitor the root resorption of the teeth.
Judicious weighing of risks and benefits is recommended before commencing orthodontic treatment because each case of SRA will pose unique challenges to the clinician. In case of mobility of the affected tooth/teeth, orthodontic treatment might not be indicated. Asymptomatic teeth however can be moved orthodontically keeping tooth movement to a minimum.
Using light forces throughout the treatment by having longer intervals between activations and appointments will ensure better stability in the long term.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to thank Prof Dr Abdul Rashid Haji Ismail, for the relentless support and encouragement in the publication of this case report as well as the Department of Oral Radiology for the expert services offered.
References
Footnotes
Contributors RRP contributed to the documentation, manuscript writing and correspondence. RSS was involved in manuscript writing, editing and submission. VSN contributed to imaging and investigations. MM contributed in manuscript editing and submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.